A year later, a patient returned with an unlikely outcome and positive feedback. But, let us not be so naive to think the impact of clinician is always positive. Sampling bias is not always bad I guess, I’m lucky she walked into the medical ICU that day. Hopefully, the impact of her visit will last past tomorrow. Clinicians, after all, are human as well.
I wondered to myself about how easy it was to treat, interact, and generally be pleasant to this patient and her husband. Not that her case was simple, or her progress quick, but the interactions with family, the social aspect was nearly effortless. And, she was full of gratitude and positive energy. Every clinician, at some point, experiences cultivating a strong therapeutic alliance and connection with a patient. Why? It’s likely a complex interplay between personalities, the situation, the patient’s psychological state, and the clinicians current demeanor. The perfect storm. Naturally, variance occurs in our own attitudes, performance, and interactions. Despite her struggles, her long journey, her complications, a surprising lack of complaints, in fact none, were aired. It was the patient room you never dreaded entering. Is it possible I benefited more from the therapeutic interaction than the patient and family?
I also wonder about the patients, the people who are challenging to engage. Those without social support and coping mechanisms. High symptom burden and remarkable distress. Pain. Lack of understanding. Unmet desires or requests. No resources. Learned helplessness. The patient room everyone dreads entering. Difficult, non-compliant, lost causes…or so some would say. How does the previous story end if they return for a hospital visit? I shudder at the potential. Post traumatic stress. Resentment. Acquisations. Confusion. Anger. Sadness. Loss. Depressive symptoms. What happens to those patients? Likely we see them again. By we, I mean the healthcare system. I’d postulate those are patients with a higher degree of medically unexplained symptoms, poor functional status, readmissions, poorly managed chronic conditions, and other complications. I’m sure they never volitionally come back to “visit” and tell their story, unless it’s during another hospitalization. Although, I wish they would, because it’s a narrative all healthcare professions should attend to. It’s easy, and I sense commonplace, to blame the patient in those exceedingly difficult circumstances. We’ve seen other patients do better. We’ve seen other patients understand. We’re trying our best with the knowledge and skills we possess. Why isn’t this person improving? Unfortunately, in such situations, neither the patient nor the providers are likely well equipped to deal with, rectify, or even improve the situation. What can be done to modify our education and approach to such difficult patient scenarios?
Despite the satisfying and motivating effect of this specific patient visit, I’m not sure my personal day to day practice will evolve much from the experience. Hopefully, it remains a reminder on the potential, and long lasting impact of our interactions. Hopefully, it doesn’t lead to arrogance. Hopefully, I can muster the focus and resolve to remember not everyone returns with a happy ending. And, those patients, the difficult ones, need our help too…arguably even more so. I hope I don’t forget the instances, well actually the people, that the system and myself failed…not by direct fault or intent, but because of the convoluted, complicated, regulated, inexact, and at times rushed human enterprise we practice within. Healthcare. Humans trying to take care of other humans.
Science advances by discovering new things and developing new ideas. Few truly new ideas are developed without abandoning old ones first. As theoretical physicist Max Planck (1858-1947) noted, “A new scientific truth does not triumph by convincing its opponents and making them see the light, but rather because its opponents eventually die, and a new generation grows up that is familiar with it.” In other words, science advances by a series of funerals. Why wait that long?
WHAT SCIENTIFIC IDEA IS READY FOR RETIREMENT?
Ideas change, and the times we live in change. Perhaps the biggest change today is the rate of change. What established scientific idea is ready to be moved aside so that science can advance?
The lesson of much contemporary research in judgment and decision-making is that knowledge— at least in the form of our consciously accessible representation of a situation—is rarely the central factor controlling our behavior. The real power of online behavioral control comes not from knowledge, but from things like situation selection, habit formation, and emotion regulation. This is a lesson that therapy has taken to heart, but one that “pure science” continues to neglect.
So, in knowing that knowing is not nearly sufficient, what are we to do? Metacognition, reflective experience, and recognition of incentives are components of improving our decision making performance. Studying cognitive bias, behavior change, and philosophical argument also aid critically thinking. Beyond our own personal, and professional, growth these concepts are salient within clinical practice, patient care, research, and education.
The problem with “a” gene-environment interaction is that there is no gene that does something. It only has a particular effect in a particular environment, and to say that a gene has a consistent effect in every environment is really only to say that it has a consistent effect in all the environments in which it has been studied to date. This has become ever more clear in studies of the genetics of behavior, as there has been increasing appreciation of environmental regulation of epigenetics, transcription factors, splicing factors, and so on. And this is most dramatically pertinent to humans, given the extraordinary range of environments—both natural and culturally constructed—in which we live.
Sapolsky’s essay illustrates complexity and interaction. While simplicity is important, caution is warranted to avoid over generalization. And, of course, do not discount the effect of dependency. Everything depends; on incentives, environment, previous experience, the current situation, and more. Some factors, and influences, likely have not even been identified. This is especially true in the realm of humans and behavior. An interesting book The Dependent Gene: The Fallacy of Nature vs. Nurture is an in depth exploration and refutation of inaccurate understandings of genetics.
But science still revolves, most fundamentally, around a search of the laws that describe our universe. And the one thing that Big Data isn’t particularly good at is, well, identifying laws. Big Data is brilliant at detecting correlation; the more robust your data set, the better chance you have of identifying correlations, even complex ones involving multiple variables. But correlation never was causation, and never will be. All the big data in the world by itself won’t tell you whether smoking causes lung cancer. To really understand the relation between smoking and cancer, you need to run experiments, and develop mechanistic understandings of things like carcinogens, oncogenes, and DNA replication. Merely tabulating a massive database of every smoker and nonsmoker in every city in the world, with every detail about when they smoked, where they smoked, how long they lived, and how they died would not, no matter how many terabytes it occupied, be enough to induce all the complex underlying biological machinery.
Physical therapy likely under utilizes big data and available data sets. None the less, big data inherently contains all the methodological issues of any study or data set: sampling bias, reliability, validity, blinding, confounding factors, operational definitions, and control. Remember, garbage in = garbage out. Big data must be put into context, and properly analyzed. What question is being posed? What questions can the data actually answer? And, what are the limitations? Quantity in data is never a direct substitute for quality. As Marcus asserts, “we should stop pretending big data is magic.” Data, after all, is just data, and is nothing without analysis. Analysis, if conducted improperly or with bad assumptions, breads false interpretation.
That a theory of mental illness should make reference to the world outside the brain is no more surprising than that the theory of cancer has to make reference to cigarette smoke. And yet what is commonplace in cancer research is radical in psychiatry. The time has come to expand the biological model of psychiatric disorder to include the context in which the brain functions. In understanding, preventing and treating mental illness, we will rightly continue to look into the neurons and DNA of the afflicted and unafflicted. To ignore the world around them would be not only bad medicine but bad science.
The direct parallels to physical therapy are striking. Psychological, contextual, and social factors are now recognized as foundational contributions to symptoms, function, intervention mechanisms, and treatment response. How will education, clinical practice, and research evolve to accommodate such insights?
However, limiting the potential contributions of informally trained individuals to the roles of data-collector or data-processor discounts the abilities of citizen scientists to inform study design, as well as data analysis and interpretation. Soliciting the opinions of individuals who are participants in scientific studies (e.g., children, patients) can help traditional scientists design ecologically valid and engaging studies. Equally, these populations might have their own scientific questions, or provide new and diverse perspectives to the interpretation of results.
There is a growing need for individuals to occupy the historically ill defined black box between research science/academia and clinical practice. Further, healthcare yearns for clinicians approaching patient care, clinical data collection, and clinical care from a scientific lens. Scientific and clinical research is challenging, time consuming, and expensive. Well trained, highly skilled researchers and scientists a requirement, I won’t argue otherwise. But, interpreting and translating such knowledge into clinical practice is an often under appreciated skill set. And, formal academic or clinical roles devoted to this necessary bridge are sparse. Conversely, formal means of translating clinical practice, clinical data, or even clinical observations into research (or to academia in general) are lacking. Well designed quality improvement projects are a means of fusing clinicians and scientists, clinical care and research. Yet, many clinicians lack the time and expertise to design projects, ensure proper data collection, analyze, and write manuscripts. Despite this clinicians (and academics) must: ask questions, collect data, and collaborate. We all have a role to play in knowledge creation and translation.
There is, of course, an alternative and very plausible source of big effects: Many small explanations interacting. As it happens, this alternative is worse than the wrong tree—it’s a near-hopeless tree. The wrong tree would simply yield a disappointingly small explanation. But the hopeless tree has so many explanations tangled in knotted branches that extraordinary effort is required to obtain any fruit at all…
…the world has large problems that demand ambitious scientific solutions. Yet science can advance only at the rate of its best explanations. Often, the most elegant ones are clothed around effects of modest proportions.
Physical therapy, as a profession, appears to fall victim to the search for big explanations. The factor, the intervention, the mechanism, the tool, the explanation. But, pause and appreciate the complexity of the therapeutic process. It’s complicated, it’s dynamic, and it takes time. Therapy interventions, inherently, must be the result of a multitude of smaller factors interacting, for better and for worse, to produce effect.
Immediately, I’m reminded of the effective philosophical tool of Occam’s Razor. Now, many misquote Occam’s assertion as the simplest explanation should always be favored. But, there is an often missed subtlety to the Razor originally sharpened by William of Occam. The premise is that the hypothesis with the fewest assumptions should gain favor, not necessarily the simplest. Often, the more complicated the hypothesis the more leaps of logic, and thus, the greater the number of assumptions. But, remarkably simple explanations may rely on astounding, and even grossly inaccurate, assumptions. Or worse, may be initially founded upon a false premise upon which all subsequent assumptions are, to some extent, wrong.
Occam’s razor is a great tool when used as originally designed. Unfortunately, many scientists have turned this simple tool into a fetish object. They pursue simple explanations of complex phenomena as though parsimony were an end in itself, rather than a tool to be used in the pursuit of truth.
Don’t make unwarranted, unfounded assumptions. But, be wary also of oversimplification. Simple is nice, but accuracy is better. It’s complicated after all.
But nowadays the world, and especially the world of the social sciences, is increasingly in love with statistics and data science as a source of knowledge and truth itself. Some people have even claimed that computer-aided statistical analysis of patterns will replace our traditional methods of discovering the truth, not only in the social sciences and medicine, but in the natural sciences too.
I believe we must be careful not to get too enamored of statistics and data science and thereby abandon the classical methods of discovering the great truths about nature (and man is nature too).
Statistics, despite being a field of study, are merely a tool. And, thus are prone to be misused, abused, and misunderstood.
It was designed to help researchers distinguish a real effect from a statistical fluke, but it has become a quantitative justification for dressing nonsense up in the mantle of respectability. And it’s the single biggest reason that most of the scientific and medical literature isn’t worth the paper it’s written on.
When used correctly, the concept of statistical significance is a measure to rule out the vagaries of chance, nothing more, nothing less…
Nevertheless, even though statisticians warn against the practice, it’s all too common for a one-size-fits-all finding of statistical significance to be taken as a shortcut to determine if an observation is credible—whether a finding is “publishable.” As a consequence, the peer-reviewed literature is littered with statistically significant findings that are irreproducible and implausible, absurd observations with effect sizes orders of magnitude beyond what is even marginally believable.
Beyond the misuse of significance mentioned, the concept of clinical significance is also important. Statistical significant alone can not support clinical significance, or clinically meaningful effect. And, paradoxically, apparent clinically meaningful effects are not sufficient for statistical significance. Partially, this is why research attempts to construct minimally clinical important change (MCIC) or difference (MCID) for certain measures. Although, even this concept is likely elastic. But, at the foundation of the entire issue, is the misunderstanding and misapplication of statistical significance.
Every last serious and systematic speculation about the world deserves to be preserved. We need to remember how we got to where we are, and we’d like the future not to retire us. Science should look to literature and maintain a vibrant living history as a monument to ingenuity and persistence.
I’d contend that more than a few ideas within physical therapy are ready, in fact likely over due, for retirement from discussion and clinical care. What are they? And, how do we guide them into the history books and out of our text books? Can we pay our respects to these ideas by identifying the potential mistakes within them? What lessons could be learned without perpetuating artificial relevance and unwarranted influence?
At the 2014 APTA Combined Sections Meeting in Las Vegas, during the Orthopaedic Section membership meeting, Dr. Catherine Patla stood up and expressed a notion to the Section’s Board of Directors. She was concerned physical therapists were giving away their hands (she also expressed a similar concern to the AAOMPT Executive at AAOMPT 2014). After over a year of consideration and contemplation, I have to agree. We are in the midst of a silent crisis of physical therapy scope of practice!
Motivated by Dr. Patla’s observations and concerns, I began keeping unofficial (and admittedly unscientific score) of students in my musculoskeletal programs and how their clinicals handled, well, the hand. Conservatively, about 50% of the students reports that they were expressly forbidden by clinic policy to treat hands, elbows, and to a lesser degree, shoulders. Concernedly, the distal upper extremity appears to be the land of the OT.
This is a complicated situation.
A Handsomely Negative Impact
From a profession-wide perspective, there’s not much that can easily be done to counteract clinic-level policies. Certainly, both Occupational Therapy and Physical Therapy are qualified to perform rehabilitation to distal upper extremity injuries. Furthermore, I think the ultimate care pathway, for many injuries common to the area, involves both professions. I’ve not actually met a member of either profession who thinks differently (or at least admitted as such), yet the policies exist.
This trend has potential long-term, and wide implications. From my perspective as Director of the Kaiser Hayward Physical Therapy Fellowship in Advanced Manual Therapy, this increases the challenge to train fellows, who by decree, must have experience treating and managing patients with distal upper extremity diagnoses. Outside of residency/fellowship training, new professionals may exist without ever getting to see a hand patient in some clinics/regions! Over time, the collective knowledge of physical therapists will be diluted and will atrophy. Soon no one will be left to TEACH the hand. At my previous University, it was common practice for the senior orthopaedic PT faculty to contract an OT to come in and teach the hand to DPT students. This was a constant and disappointing source of stress for me. What message does this send! We could literally be voluntarily cleaving off an important scope of our practice! The irony is, it’s the body region most important to how we treat! It’s decidedly more difficult to be a PT if you don’t have hands.
The Hand Rehabilitation Section
I don’t know any more than a couple people in the Hand Rehab Section of the APTA. Perhaps that’s my issue. Perhaps it’s because the Section itself is a bit of an anomaly. Of the 18 Sections within the APTA, it’s the only one designated by an anatomical focus. The other sections are delineated by practice areas like Orthopaedic or Neurologic, settings like Home Health, Acute Care, or Aquatics, or related professional activities like Research, Education, and Federal Advocacy. Arguably, the Women’s Health section is anatomically focused, but in fact it’s not, since Women’s Health is more broad than a pelvic floor and I think “The Vagina Section” would offer some terribly difficult search engine optimization challenges! I do not know the history of how the Hand was excised from the rest of the Orthopaedic Section and would love to learn.
All that criticism on name/organization aspects aside, you have to also argue that the Hand Section is doing the best it can with the membership audience it has (~472 members and 36 Facebook likes). It offered an outstanding selection of programming at this years CSM Meeting in Indianapolis. Everything from a high-profile lecture including ESPN’s Stephania Bell, to a comprehensive clinical reasoning model for TFCC management by Brenda Boucher and Pieter Kroon was offered. Notably, the Hand Rehab Section also offered two pre-conference courses and presented the results for projects for 3 different clinical practice guidelines: carpal tunnel, distal radius fractures, and lateral epicondyalgia. Yet, while all this is taking place, other PT’s seem more than happy to give up the hand and let someone else manage it. Let some other PROFESSION manage it.
Hands are for Holding
To me, this boils down to a grassroots effort, and is an issue of personal responsibility as a professional. You cannot in good conscious, let your clinic enforce and carry out a policy that prohibits, or through practice, eliminates the opportunity to treat any body region, especially the hand. We all know the outcry when outside professions claim a technique is only their purview, and attempts are made to remove that from our practice. Physical therapists rise up in a collaborative rage and claim it back. Yet, I see malaise and laziness, and an acceptance of insufficient knowledge as a behavior pattern among physical therapists in these clinics. That may seem harsh, but I can’t see it any other way.
My one caveat, and an important one at that, is that some hand injuries do require a very experienced hand specialist. Hand tendon surgical repairs quickly surpass entry-level practice. There is an insufficient numbers of physical therapists trained Certified Hand Therapists. In fact, I have only encountered one PT who holds the dual acclaim of Fellow of the Academy of Orthopaedic Manual Physical Therapists AND is a Certified Hand Therapist: the aforementioned, Dr. Boucher, who hails from Texas State University and teaches as part of the Manual Therapy Institute’s manual therapy fellowship program.
There are pathways, and opportunities that can happen, and I’ll outline my suggestions in just a moment, but this boils down to each and every physical therapy professional deciding to hold onto hands. It’s up to YOU!
Getting a Grip on this Problem
By all means, this is just a suggestion, but we need to start somewhere and why not now? Please comment, edit, innovate, or ACT on this:
Hand Rehab education should be led by physical therapists as often as possible in DPT programs.
Individual PT’s in clinics with hand-prohibitive policies should challenge these, and reach out to professional advocates like those in the Hand Rehab Section for assistance if needed.
Consideration of upper extremity policies in DPT Clinical Education should occur.
Joint clinical practice guidelines should be developed by OT’s and PT’s collaborating as authors.
Increased visibility and ultimately membership in the Hand Rehab Section. 36 Facebook likes is not going to cut it. 472 members is difficult to defend.
Development of post-professional pathways for Hand/Wrist/Elbow instruction including residencies, fellowships, and some stake in the Certified Hand Therapist credential.
Consideration of how the Hand Section can further collaborate with the Orthopaedic Section (absorbed by the Ortho Section?) and AAOMPT to further their collective mission.
Wide APTA support for these endeavors, including resources for training training, pathways for expertise, research, and advocacy.
Thanks for listening. Thanks for thinking. Thanks in advance for taking the challenge to not let this problem get any worse!
Atul Gawande, MD, MPH is a surgeon, writer, and researcher who provides genuine insights into the challenging complexities of medicine. But, he also creates novel solutions like check lists in operating rooms. Dr. Gawande connects reflection on personal experience, processes from other fields, and scientific research like IL-10 immune modulation into insightful narratives that outline the rationale and concrete action needed for improvement. He contends problems in healthcare are not necessarily conceptual, but rather stem from poor processes. There is a lack of knowledge translation and application. In his book Better: A surgeon’s notes on performance, he explores the science of performance and specific high performing individuals. At the end, he outlines general advice for improvement. Atul Gawande’s suggestions for becoming a positive deviant:
1. Ask an unscripted question
Ours is a job of talking to strangers. Why not learn something about them? On the surface, this seems easy enough. Then your new patient arrives. You still have three others to see…But consider, at an appropriate point, taking a moment with your patient. Make yourself ask an unscripted question. So ask a random question of the medical assistant…a nurse you into on rounds…you start to remember the people you see, instead of letting them all blur together. And sometimes you discover the unexpected. If you ask a question, the machine begins to feel less like a machine.
2. Don’t complain
We all know what it feels like to be tired and beaten down. Yet nothing in medicine is more dispiriting than hearing doctors complain. Medicine is a trying profession, but less because of the difficulties of disease than because of the difficulties of having to work with other human beings under circumstances only partly in one’s control…You don’t have to be sunny about everything. Just be prepared with something else to discuss: an idea you read about, an interesting problem…
3. Count something
Regardless of what one ultimately does in medicine–or outside medicine, for that matter–one should be a scientist in this world. In the simplest terms, this means on should count something.
4. Write something
It makes no difference whether you write five paragraphs for a blog, a paper for a professional journal, or a poem for a reading group. Just write. What you write need not achieve perfection. It need only add some small observation about your world. You should not underestimate the effect of your contribution, however modest.
5. Change
Look for the opportunity to change. I am not saying you should embrace every new trend that comes along. But be willing to recognize the inadequacies in what you do and to seek out solutions. As successful as medicine is, it remains replete with uncertainties and failure
Simple, applicable, and needed suggestions.
To be sure, we need innovations to expand our knowledge and therapies, whether for CF [Cystic Fibrosis] or childhood lymphoma or heart disease or any of the other countless way sin which the human body fails. but we have not effectively used the abilities science has already given us. And we have not made remotely adequate efforts to change that. When we’ve made a science of performance, however–as we’ve seen with hand washing, wounded soldiers, child delivery–thousands of lives have been saved. Indeed, the scientific effort to improve performance in medicine–an effort that at present gets only a miniscule portion of scientific budgets–can arguably save more lives in the next decade than bench science, more lives than research on the genome, stem cell therapy, cancer vaccines, and all the other laboratory work we hear about in the news. The stakes could not be higher.
More specifically to physical therapy within the realm of healthcare, two of the most profound, if not obvious, examples are the “treatment” of musculoskeletal conditions (pain) and the mobilization of hospitalized adults. The knowledge is present to dramatically improve both. Societally, there is dire need for more movement, whether activity or exercise, in healthy individuals as well as older adults, those with chronic medical conditions, and cardiac & pulmonary disease. Again, the knowledge is there. But, are the processes and incentives for performance available? How can physical therapy as a profession and each of us as individuals move forward to enact meaningful change? Atul comments:
True success in medicine is not easy. It requires will, attention to detail, and creativity. But the lesson I took from India was that it is possible anywhere and by anyone. I can imagine few places with more difficult conditions. Yet astonishing successes could be found. And each one began, I noticed, remarkably simply: with a readiness to recognize problems and a determination to remedy them.
Arriving at meaningful solutions is an inevitably slow and difficult process. Nonetheless, what I saw was: better is possible. It does not take genius. It takes diligence. It takes moral clarity. It takes ingenuity. And above all, it takes a willingness to try.
Ask questions. Sideline complaints without solutions. Count things. Write. Change.
Are we teaching it backwards? Without understanding premise or argument validity in relation to research, an individual article analyses may be useless. A study may be flawed on premise alone even with strong methodology and statistically significant results. A valid argument is false. And, inappropriate conclusions will be drawn. Likely, this will lead to misguided justifications and explanations. Such errors can affect clinical practice, education, and future research.
Plausibility must not only take into account previous clinical research and outcomes studies (efficacy and effectiveness), but also basic science and current mechanistic research. Such an approach prevents reinforcing an unlikely or inaccurate explanatory model despite positive outcomes. Unfortunately, physical therapy is likely plagued by positive outcome studies misinterpreted, and thus explicitly or implicitly, supporting a theoretical construct that is (may be) invalid. One example, more specifically, is the variance in explanatory models of manual therapy effect.
What are my beliefs? Biases? Preferred treatment constructs and approaches?
An overlooked area of assessment is ourselves. The person doing the analyzing. It’s imperative that the critical lens of analysis be pointed back upon its user. Rarely will an orthopedic manual physical therapist postulate that manual therapy does not work. The very best may ponder if the mechanisms are completely outside the current understanding. A physical therapist practicing in an ICU rarely questions the effectiveness of movement and mobility. But, clinicians and researchers should strive to rigorously falsify via the scientific method in order to focus accuracy and understanding over time. Physical therapists are inherently, and understandably, focused on the specifics of treatment that appear most important. What exercise? What technique? What works? Yet, the scientific rigor, and uncomfortable thought, of attempting to prove physical therapy does not work will lead to more specific knowledge on why it does work and the potential attainable outcomes. Seems contradictory, but falsifiability is the basic tenant of hypothesis testing in science. So, ask yourself: what would it take to change my mind? It’s time for some serious critical thinking.
Points to Ponder
Hypothesis & Null Hypothesis
Plausibility of Hypothesis based on previous research and overall knowledge
Methods Critique (utilize checklists)
Efficacy vs. Effectiveness Design
What is the comparison or control group?
Are these groups similar in abstract variables such as frequency, duration, and one on one time?
Believability of the comparison or placebo by patient?
What the results can tell us given study design
What the results can NOT tell us given the study design
Plausibility of results from author’s interpretation
Plausibility of theoretical model presented or utilized
Plausibility of the discussion & conclusion in relation to understanding on the topic specifically
Plausibility based on basic science, physics, mechanics, including tissue mechanics, physiology, psychology
How else could the results be explained? Placebo? Regression to the mean? Different mechanisms?
Did the authors make the appropriate conclusion?
What’s YOUR conclusion and understanding?
Overall summary and critique
How and why to integrate?
What is the take away?
“That’s valid,” you say, but what do you mean by that? A single statement can be valid by itself if it is a previously proven “truth”, but what about an argument? You remember arguments, right? Premise, premise, therefore conclusion? Funny thing about valid arguments, they have nothing to do directly with truth. Arguments can be valid and false at the same time, just as they can be invalid and true at the same time. What?
Since deductive arguments are the basis of all research, you need to understand this concept. I have quoted before on a podcast, “A flawed study is still a flawed study regardless of p-value or level of evidence. – Erik Meira, When a valid argument can be false
It is reflective and complex decision-making that integrates all sources of evidence that we should be having serious conversations about, and its that thoughtfulness [PDF] that is required of a doctoring profession – not the myopic and obtuse yes or no to the question: “Are you evidence based?” – Jason Silvernail, DPT, DSc
Conceptual variation is more damaging, and a bigger issue, than perceivable, apparent practice variation. Because of the multi-faceted nature of the mechanisms of effect in physical therapy treatments, especially for pain, striving for observable decreases in “practice variation” may not actually solve many of the issues within the profession. The real problem is conceptual differences. The stark contrast between explanatory models, and stories told, results in significant variance in explanation and education received by patients. Patients are still routinely told they have “bad” posture, an SI joint that is “out” and weakness causing their painful problems. Such unhelpful and debunked ideas are the unnecessary imaging of our profession.
Now, to be fair, striving for a decrease in practice variation within physical therapy is a worthwhile endeavor. However, I am not convinced current conceptualizations are the appropriate approach. Assessing variation in medical treatments and practice is likely easier than in physical therapy practice. Why? It’s more concrete. Medical treatment relies heavily on the appropriate diagnosis of essential, or substantial diagnoses. Treatment follows, and is mostly dependent on proper diagnosis. Thus, analysis of timely proper diagnosis, matching of treatment and diagnosis, and actual treatment content is more concrete to study. For physical therapy, a different construct is required. The complexities of the clinical encounter and individual nature of the therapeutic process in conjunction with the many potential and identified mechanisms of treatment effect complicate the study of variance. Striving for utilization of the exact same interventions is likely to be a surface level success. It appears like progress. Therapists are dealing with many nominal diagnoses and messy concepts such as unexplained symptoms, function, and behavior change. (note: medical diagnosis is still very complex and full of challenges)
Specificity should be sought after, but not assumed. As more is understood about the effects of interventions it is becoming apparent that techniques, exercises, and interventions themselves are not as specific as originally assumed. If observably clinicians appear to have no practice variation, but utilize different conceptual frameworks and tell the patient in front of them different stories, gross variation is actually still present. Utilization of similar constructs may result in similar “outcomes,” but with significantly different “interventions.” So, what are the common factors?
Regardless of setting, physical therapists should strive for the most accurate deep models of practice, validated and efficient processes in conjunction with an individualized, assessment based, response dependent approach. The best clinical research evidence should be incorporated. This will lead to less practice variation, you just might not be able to see it. Observational variation in interventions may not actually represent difference in concepts. Conversely, two clinicians may perform exactly the same “interventions” with marked disagreements in conceptual framework, reasoning, patient interaction, and patient education. Maybe the method is not the trick? Maybe the process is as important as the product? It’s high time for the accountable practitioner. That means metacognition, critical thinking, and science based practice. Simple…now only if it were easy.
An incentive is something that motivates an individual to perform an action.
And, that something could be anything. Meet the omnipresent influencer of behavior. Frequently, incentive is understood to be associated with some form of monetary compensation for specific behavior. But, incentives are not merely monetary. And, they exhibit influence. Yes. Always. 100% of the time. In any environment, any scenario, any interaction, and every decision including clinical encounters. Incentives can be viewed as any tangible or intangible reinforcement, and thus influencer, of behavior. Theses “rewards” range from monetary to personal, concrete to cognitive-emotional. And interestingly, incentives still affect behavior even when individuals consciously identify and recognize their presence. They are social, contextual, or even cultural. And, they impact decisions and performance.
Incentives are present in a variety of forms and contexts. Most generally, incentives can be assessed via a variety of binary comparisons including: Explicit verses Implicit, Reward verses Punishment, Short verses Long Term, and Immediate verses Delayed. Yet, the content of incentives range from monetary to verbal, and in contexts of private and public. The environment, including people, specific location, and context of the situation, in conjunction with broader constructs such as expectation and culture also matter.
Physician’s prescribing habits are affected by pharmaceutical marketing. Prescribing is affected by the gifts, no matter how menial, of pharmaceutical companies. This effect is observed even if physicians believe the gifts have no bearing on their prescription decisions. The data and incentives lead the Office of the Inspector General to research gifts and payments that promote prescription drugs. In this instance, physicians are Prescribing Under the Influence:
This kind of advertising is crucial to sales. A doctor is not going to prescribe something he or she has never heard of, and it’s the drug representative’s job to get the products’ names in front of the physicians. Maybe the drug representative does that while the resident is slathering cream cheese on a bagel; maybe it’s while the intern is saying, “Oh, what’s this cute little stuffed bear?” Either way, the doctor stops and spends a moment.
In private practice, the little gifts are often even more important. If you’re a drug representative, physicians are usually not interested in talking to you unless you have something to catch their attention. Then you can get your three sentences in: “We’ve got such and such on the hospital’s formulary now.” Or “The new form of this drug can be given once a day instead of four times a day. The patients will love it.” It’s a way to get in the door so that your information rather than somebody else’s reaches the doctor’s brain.
Self-referral, or referral for profit, is associated with increased utilization of lab tests, imaging, and physical therapy. A meta-analysis revealed a 2.48 combined relative increased frequency of referral in refer for profit scenarios. In most cases, I truly believe physicians are not sitting in front of patients actively scheming on how to justify an imaging procedure, lab test, or referral to physical therapy in order to maximize profit. On the whole, I don’t assume the physicians in these scenarios are unethical and overtly over prescribing. But, the incentive is present, and thus behavior is altered. The evidence shows that self-referral invariably leads to higher utilization and higher costs.
What are specific incentives within the profession of physical therapy? What should be modified? Everyday outcome measures are handed to patients, clinical measurements made, and assessments written. What are patients and incentivized to say and do? Or, believe? Administrators, managers, and clinic directors in hospitals and private clinics present data to their staff. Specific metrics are identified and goals are constructed.
Recognizing the development of interaction between personal and environmental (including social, societal, cultural) influences on behavior illustrates the complexity of how, when, and why we behave in certain ways. In healthcare, the layers of systems and hierarchy of influence is complicated. Our decisions and behavior are not nearly as rationale, nor conscious, as they feel to us personally. The interplay of personal, inter-personal, and environmental influences coupled with tangible or perceived rewards influences how people act. In conjunction with individual motivation, incentives, both seen and unseen, are determinants of who will thrive in certain educational and clinical contexts. One such example is the difference between extrinsic and intrinsic motivation. What people do is just as complex as why people think they do it. And, there is a disconnect, a blind spot, between our perception of bias in ourselves verses others.
Unfortunately, incentives have unintended consequences. The cobra effect is an illustration that “incentives don’t always work out the way we expect them to.” Beyond identifying a target metric and outcome, it’s imperative to identify the actual behaviors that are desired. Sometimes a change in a specific measurement (productivity, patient report outcomes, etc) do not necessarily reflect the desired behavior changes. In particular, research investigating payment incentives and subsequent clinician behavior within healthcare illustrate tangible manifestations of “unintended consequences.”
How is the outpatient therapist incentivized if measured and assessed primarily via patient report questionnaires? How are we changing behavior in the acute care therapist by assessing them based on the number of “units” they “bill?” What about the outpatient therapist who receives a bonus based upon units billed? What if changes in the metrics we are utilizing don’t truly illustrate significant change, don’t result in the best care, and don’t reinforce ideal behavior? A health services research article on medicare payment comments:
While some payment methods may lead to excessive utilization, other payment methods may put too much pressure on cost containment and potentially lead to underprovision of resident care (Coburn et al. 1993; Cohen and Spector 1996; Murtaugh et al. 1988)
In addition to tracking specific measures, ideal behaviors need to be identified. To account for unintended consequences broadly identify various behaviors likely to lead to the measured goals. Sometimes behaviors that are actually not desired can cause significant desirable change in target measures. Undesirable action for desired outcome. So, what behaviors can cause a change in the metric? And, what contributes to encouraging such behaviors? But, also, what incentivizes behaviors that change the metric, but may also cause unintended consequences?
If a clinic, hospital, profession, or health care system seeks to fundamentally alter care delivery robust assessment of the current incentives within healthcare, including conflicts of interest is mandatory. Then change the incentives to affect and encourage ideal clinician behavior. A successful approach likely involves a combination of incentivizing important outcomes as well as specific behaviors. Changing the single data point does not necessarily reflect the desired overall change in other measurements or behavior. The depth of affect of incentives in conjunction with unintended consequences illustrate the difficulty in controlling change. A seemingly brilliant idea such as “pay for performance” or outcomes based payment is fatally flawed without a conscientious focus on the many potential behaviors that may result in the specific outcome. Might it even be chaos?
What are the incentives? Identify the answers and then target behaviors requiring alteration. Shift behaviors towards ideal processes. Ideal behaviors will likely have positive unintended consequences. A myopic focus on only the desired numeric change will produce a myriad of potentially paths to “success.” Some of these paths were never the intended action of success. And in fact, may be the opposite of the incentive’s initial philosophical goal.
What I couldn’t say – but wanted to – was the truth: I don’t care.
Seriously. I don’t. I can’t.
Keith P states “I don’t care.” And, I think he’s right. A certain type of detachment from the potential suffering and emotional struggles of patients is vital for a clinician. The ability to assess, analyze, and make proper decisions may be clouded if those treating are overly emotionally involved in the circumstances of those they treat. Further, shouldering the burden of the many unfortunate clinical, emotional, and social situations encountered within healthcare can easily leave one with a sense of hopelessness. It’s quite easy to succumb to pessimism and apathy when the grand scale of suffering, inequality, and just plain bad luck occupy the beds and treatment tables daily. But, is this ideal for patient interaction? What do patients prefer? Establishing and enhancing alliance, rapport, and an environment of care is necessary. An explicit connection with the patient is a precursor to, or maybe even the foundation of, the therapeutic process. Too far to one extreme and the risk is burnout. Too far to the other and the risk is a cold, distant clinician (and still burnout). As in anything, explicitly defining terms and concepts is helpful.
Definitions and Terms
Sympathy, empathy, compassion, and caring are connected concepts, but have differing definitions. And, specifically within healthcare these concepts require more specific exploration. While various, and vague, characterizations of sympathy exist within and outside of healthcare, for the sake of clarity sympathy generally centers around an emotional state of feeling. It can manifest as pity or sorrow for another, a common feeling, or a relationship in which that which affects one mutually affects the other. The simplest definition is entering into or sharing the feelings of another. Empathy, by contrast, is characterized by identification and understanding. But, empathy has been sub-characterized into two, or even three, separate conceptualizations: emotional (or affective), cognitive, and compassionate empathy. To complicate matters, compassion itself is an awareness of suffering of another and a desire to act in order to relieve it. Therefore, compassion is best understood as an action, or potential action. This desire and subsequent action may stem from both rationale and emotional sources.
Healthcare & Empathy: Emotional vs. Cognitive vs. Compassionate
Daneil Goleman briefly outlines and discusses the three (potentially) separate kinds of empathy. Empathy is founded upon understanding and identification which may include projecting ourselves (hypothetically) into another’s situations. And, it can happen emotionally and/or cognitively. Emotional empathy is the ability of a person to feel a similar emotion as another (which confusingly can be accomplished cognitively). Although this appears to mirror sympathy, sympathy is a sharing of emotion, or emotional state, feeling along with another. In contrast, cognitive empathy relates to recognizing, understanding, or even appreciating a person’s feelings. To be fair, the definitions of sympathy and empathy as well as cognitive verses emotional empathy appear to overlap. It seems they are, at times, used interchangeably. Specifically to healthcare, empathyis “a cognitive attribute that involves the ability to understand the patient’s inner experiences and perspective and a capability to communicate this understanding,” Many in healthcare education recognize IQ and didactic skill are only a portion of the ideal clinician equation. The ability to understand and perform within the above constructs relates to emotional intelligence. And, “…empathy, as defined here, must be included in the curriculum. It is a powerful communication tool that enables a clinician to clearly express his or her understanding of another’s suffering while protecting his or her own psychological integrity.”
Do you have to care to be caring in your practice?
A major issue in health care professions generally, but therapy specifically, is mistaking the necessity of cognitive empathy for a requirement to sympathize and feel with patients. Front line clinician burn out is in part due to an understandable inability to sympathize with every patient, and the resulting cold, concrete distance that can result in situations when sympathy is not feasible. Whether clinician fatigue, a need for emotional distance, or carryover from the patient before feeling the emotions, sympathizing, and providing pity to every patient is likely not possible. And, probably not effective. The issue is likely further clouded by a lack of understanding regarding the differences of sympathy and empathy. I don’t ever remember learning about this stuff. But, it’s vital. The concept of objective empathy grossly changed how I approach patient interactions. Patients and practitioners report “compassionate care” is important to successful medical treatment. So, what’s to be done?
The role of the clinical instructor is paramount in helping students to become aware of behaviors that can block empathy. We can no longer simply hope that our students will become mature professionals with compassion and empathy for patients. We must create experiences to develop these attributes, and we must take responsibility for modeling these behaviors and reflecting on them with students, to raise their consciousness about the nature of a mature healing presence.” The art of healing is, in part, made up of a therapeutic use of oneself or a therapeutic presence for patients. This presence is more than knowledge and skill alone; it is also composed of a compassionate understanding of the patient and a communication that the therapist is worthy of the trust that the patient has bestowed. Empathy enhances the therapist’s therapeutic presence and deepens the patient practitioner interactions without fear of losing one’s self in the process. This shared meaning seems to enhance the patient’s process of healing. Carol Davis, Can Empathy be taugh? PTJ, 1990
To the observer I’m sure it appears I do care, and care deeply. But, in the end Keith, you’re right. I don’t care. And, I don’t need to. Does that mean I never engage with patients on an emotional level? That patient’s circumstances never affect me? That I never feel a connection, or shared emotional states with a patient? Or, a powerful emotional response during the course of treatment? Of course not. It happens. And, that’s OK. But, we don’t need to strive for it. Someone inquired to Keith “I wonder if being detached from our patient makes for a better clinician… Any thoughts?” He responded:
A therapist needs an appropriate amount of attachment for success, but that attachment, I reason, needs to be to a high professional standard of care, not the patient’s outcomes themselves.
You don’t need to sympathize to provide appropriate empathy. You don’t need to care to be caring. You don’t need to feel the emotions of your patients to address the emotions they feel.
When I freed myself from the responsibility for the “outcome” of the clinical encounter, something interesting happened. I freed my patients from blame, also. –Jason Silvernail
It’s important to care, but maybe not in the assumed emotional involved ways. And, I think we should not apologize for claiming not to care. I’m still, I think, a caring clinician. I just don’t make a point of feeling pity for the suffering I encounter. I am passionate, empathetic, and hopefully a thoughtful interactor.
…an older relative of mine who has cancer is going back and forth to hospitals and rehabilitation centers. I’ve watched him interact with doctors and learned what he thinks of them. He values doctors who take the time to listen to him and develop an understanding of his situation; he benefits from this sort of cognitive empathy. But emotional empathy is more complicated. He gets the most from doctors who don’t feel as he does, who are calm when he is anxious, confident when he is uncertain. And he particularly appreciates certain virtues that have little directly to do with empathy, virtues such as competence, honesty, professionalism, and respect. –Paul Bloom, Against Empathy
We need to be able to treat our patients, all of them, and still function in our own lives. If not, we risk riding the roller coaster of sympathy and pity in clinic at the potential expense of engaging emotionally in our personal lives. It’s a bad outcome all around. Our patients need us to understand, interact, and guide them along the best possible course of recovery. So, whatever we call it, put your pity aside. I’m not sure our patients want it anyway. Be resilient. You don’t need to care to provide compassionate care. Our patients need us to listen, but also to initiate difficult, honest conversations.
If immobility is pathology, then movement is medicine. But, now that the rationale is present, how is action initiated? Understanding the current literature in regards to mobility and physical therapists in the intensive care unit illustrates the need and the potential for physical therapists. This potential leads to the vision. Yet, rationale and vision do not guarantee action, nor results.
Every patient requires an individualized assessment and interaction to determine the best plan of care, outcomes tracking, and goals. So, does each individual ICU. Evaluation of current practice and culture, barriers to mobility and physical therapy, and a plan to achieve specific goals. Data and outcomes tracking can provide insight into progress.
Research surveying various professions elucidates commonly reported barriers to mobility and physical therapist involvement in the ICU. Yet, many of the identified barriers appear more perception than the reality. Fears based upon “what if?” scenarios. What if the patient falls? What if a line becomes dislodged? What if they decompensate? What’s the worst possible event? Illness severity, safety, and line dislodgment are commonly report. These fears are contrary to the literature on safety and feasibility. Does this indicate these concerns are likely unwarranted?
Barriers: Perception and Reality
Perception is reality. The multi-disciplinary environment of critical care, including the a culture of a specific unit, requires analysis to ensure specific perceptions are identified. Barriers should be overcome with education, discussion, training, and graded exposure. Individual practitioner’s perceptions, fears, and concerns contribute to professional interactions, unit culture, and ultimately patient care. Fear based barriers include illness severity, illness acuity, safety, feasibility, and perceived lack of benefit. Other reported challenges include lack of consults, staffing, knowledge, time, expertise, experience, cost, equipment, and unit culture. All unit specific and individually identified barriers must not only be acknowledge, but adequately addressed. Reported concerns are not to be discounted.
1. Do you think physical therapy should evaluate/screen all intensive care unit/cardiovascular intensive care unit patients?
2. Do you feel comfortable getting patients into neuro chairs without physical therapy?
3. Do you feel comfortable using the mechanical lifts without physical therapy?
4. Do you get patients out of bed/ambulate without physical therapy if they are able?
5. Do you think patients should be getting up on ventilators?
6. What are the barriers to mobilizing patients on ventilators?
7. What are the harmful effects of physical therapy working with patients in the intensive care unit?
8. What can physical therapy do to improve communication with the RNs, MDs, respiratory therapists, patients, families, etc.? Please be specific.
9. What can physical therapy do to improve patient care? Please be specific.
The survey questions revealed many of the barriers listed above. Interestingly, all respondents agreed that every patient in the ICU should be evaluated by a physical therapist.
As much, as soon, as often as we can?
The concept of mobility and rehabilitation during intensive care appears quite important and profound. Therefore, it’s quite obvious that every patient should be out of bed and ambulating at least three times per day. Well, not exactly. Although being in the ICU in the presence of lines, tubes, and life support equipment should not automatically preclude individuals from movement and therapy participation, each patient will present and perform quite differently.
So, what are the specific interventions? How does a physical therapist decide what to do? And, when? What about dosage, intensity, frequency, and duration? Similar to other patient populations (such as individuals with back pain), critical illness is far from homogenous. Even a very specific ICU type contains a range of diagnoses and individuals. Treatment content, duration, intensity, and frequency should likely vary. Further, given the acuity of illness and the medical complexity of patients, close monitoring of many variables is necessary. The specifics of these particular concepts remain complicated and dependent on many variables. At times it appears there are more questions than answers.
Generally, the goal is to decrease sedation, bed rest, and confusion while increasing wakefulness, movement, and engagement. There are nearly infinite options available to accomplish such goals. An approach of “as much, as soon, and as often as possible” simplifies the conceptualization of treatment. But, such an approach is always performed within the specific confines and constraints of the system, staffing, experience, and culture of the current clinical situation.
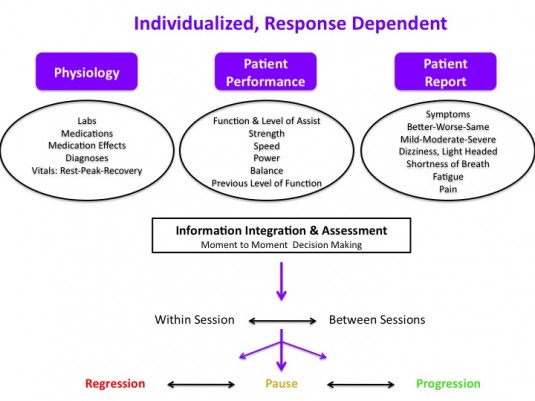
Response Dependent Progression
An individualized, response dependent approach facilitates proper monitoring from moment to moment and session to session. Decision making requires integration of information from multiple sources to reach an overall assessment that determines progression, pause, or regression. Such a system hopefully decreases the likelihood of grossly “over treating” or “under treating” a specific patient at each specific encounter. The variable nature of medical stability, presentation, and physiologic status of critical ill patients may result in robust, swift changes in vital signs, physiology, and even patient performance. A patient’s specific clinical scenario including diagnoses, physiologic state (labs, medications, vital signs), and current medical goals warrants the a priori construction of individualized safety parameters regarding upper and lower limit values for vital signs.
Response Dependent Progression. Individualized prescription & progression based upon moment to moment assessment.
An assessment of current and historic practice can include average unit census, average number of physical therapy consults, percent of the unit with consults, and number of patients actually seen per day. Average time from admit to first physical therapy encounter in conjunction with average duration and frequency of treatment provide general insights into current physical therapy practice.
Next, by assessing unit specific data in relation to current practice, predictions for future staffing, equipment, and training can be constructed. Such a model can be further specified based upon targets for the number of patients (or percentage of the unit) to be treated each day, and at what frequency. In addition, the current number (or percentage of) patients who are likely to benefit from, or be appropriate to participate in, physical therapy can illustrate a disconnect between current practice and ideal practice. Identifying a lack of consult standards may shed light on variability in consult numbers, timing, and frequency. Standardized criteria for consults, mobility, or physical therapist involvement provide assistance in decision making. But, each individual patient requires analysis within the framework of guidelines, not decisions mandated by them.
The current demand (consults), physical therapy practice, and provider perceptions are utilized to model need, illustrate the lack of physical therapist involvement, and potentially quantify a current lack of resources to provide appropriate timing, frequency, and duration of therapy. If feasible, informal or formal investigations into factors associated with physical therapy consultation provide further understanding into current practice regarding physical therapy consultation and practice. A disconnect between the research literature and current unit culture, including various professions practice patterns, highlights the need for transdisciplinary practice change and potential quality improvement.
Financial Modeling
Johns Hopkins constructed a financial model allowing prediction of staffing, costs, and potential financial outcomes. By utilizing the number of yearly admits, current ICU & hospital length of stay (for a specific targeted ICU), and direct variable costs of care a very accurate model of staffing, start up costs, and potential cost savings scenarios can be assessed. Varying possible length of stay reduction outcomes allows for a sensitive, yet conservative prediction of cost savings in multiple potential situations. Modeling various outcomes allows for the presentation of worst case, likely, and best case end points. Utilizing actual data from their own quality improvement project and data from the literature they conclude
A financial model, based on actual experience and published data, projects that investment in an ICU early rehabilitation program can generate net financial savings for U.S. hospitals. Even under the most conservative assumptions, the projected net cost of implementing such a program is modest relative to the substantial improvements in patient outcomes demonstrated by ICU early rehabilitation programs.
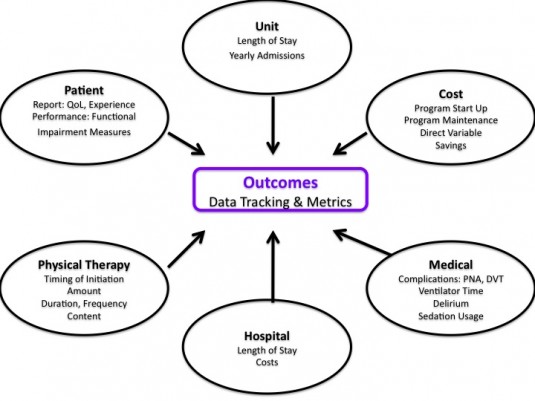
Measurement and Outcomes Tracking
The potential data and outcomes depend on data availability, program goals, ICU type, patient population as well as any specific research questions. Outcomes can be analyzed at the patient, unit, and hospital level.
Potential construct areas of measurement for ICU mobility, rehabilitation, and physical therapy programs
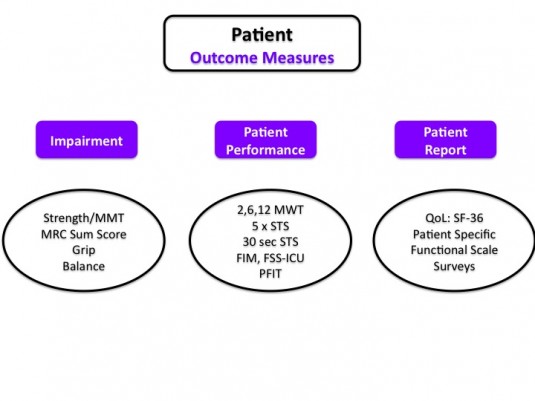
At the patient level there are a variety of impairment, patient report, and patient performance measures, many of which have been specifically investigated for utilization in the intensive care unit.
Quality Improvement Project Design
Designing and implementing a quality improvement project with a focus on research methodology improves the accuracy of measured results. Such an approach eases discussions with hospital administrators regarding need, costs, and program appraisal. Appropriate planing, background research, and project construction prior to implementation allows for more specific analysis.
Background, Construction, & Education
Assess current PT practice, unit culture, clinician perspectives
Compare current practice to ideal practice, current program models, and feasible quality projects
Construct project goals
Model staffing, training, equipment, and program requirements
Identify, acknowledge, and address current barriers
Identify champions from each discipline: PT, RN, MD, RT
Identify educational needs of PT and rehab department
Identify educational needs of other disciplines
Perform education and follow up meetings
Data
Identify target data and outcomes tracking
Obtain facility specific data for financial modeling
Build data tracking sheets & data bases (if needed)
Leverage electronic medical record (if able)
Train clinicians on documentation and “data entry”
“Go live” with documentation and data collection
Establish a post documentation training pre-project implementation baseline
Implementation
“Go Live”
Sustain & Maintain Program via Updates and Meetings
Evolve care based on observation, feedback, and data analysis
Assess & Analyze Program and Data Collected
The elegance of a quality improvement approach is the potential for an ever evolving feedback loop of assessment, planning, implementation, and analysis. At specified intervals, repeat the process based on current results, identified issues, and current research.
Facility Specific Questions and Issues
1. What if current practice illustrates a lack of consults, infrequent consults, or poor timing of consults (i.e. too late in hospital course)?
Create specific consult criteria. Educate nursing staff and physicians. Provide checklist.
2. What if there is no dedicated physical therapist in ICU?
Quality improvement project focused on unit based physical therapist and increased overall patient mobility.
3. What if patients are too sedated?
Assess RN sedation guidelines and practices. Pair therapy with sedation vacations & awakening trials. Meet with MD’s, RN’s, and RT’s. Work with RN educator to facilitate RN lead project regarding sedation.
4. What if there is a lack of patient mobility outside of therapy sessions?
5. How to prioritize if unable to address every consult and patient on caseload in the ICU(s)?
Focus on duration of bed rest, individuals requiring mechanical ventilation, especially those requiring greater than 3 days of mechanical ventilation. Assess last time mobilized and last therapy session.
Quality and Assessment
Obviously, analyzing and interpreting clinically generated data is difficult. Given the complexity of the daily clinical environment and lack of rigor available in a controlled research trial, data can often be inaccurate or even misleading if not understood properly. Utilizing a quality improvement model within the context of critical care is an evolving method for program design and interpretation, but
The results of many quality improvement (QI) projects are gaining wide-spread attention. Policy-makers, hospital leaders and clinicians make important decisions based on the assumption that QI project results are accurate. However, compared with clinical research, QI projects are typically conducted with substantially fewer resources, potentially impacting data quality…Data quality control is essential to ensure the integrity of results from QI projects.
Resources exist for appropriate design, training, data collection, implementation, sustainability, assessment, analysis, interpretation, and translation of quality improvement designs and data.
Especially when you are unaware of it’s caveats and limitations. Per Malcom Gladwell’s Outliers many advocate the 10,000 hour rule regarding the development of expertise. While this is a useful illustration of the sheer volume of practice necessary to develop mastery, it’s likely over simplistic for a concept as complex as expertise in a complicated craft.
The secret to continued improvement, it turns out, isn’t the amount of time invested but the quality of that time. It sounds simple and obvious enough, and yet so much of both our formal education and the informal ways in which we go about pursuing success in skill-based fields is built around the premise of sheer time investment. Instead, the factor Ericsson and other psychologists have identified as the main predictor of success is deliberate practice — persistent training to which you give your full concentration rather than just your time, often guided by a skilled expert, coach, or mentor. It’s a qualitative difference in how you pay attention, not a quantitative measure of clocking in the hours.
Clinical care, research, and critical thinking are no different. It is not experience, as linear measurement of time, but rather quality practice and volume that matters in developing high level skills. Left to its natural devices our brains and psyches are stubbornly prone to bias and errors in rational thinking. Confirmation bias and improper associations such as post hoc ergo propter hoc (since event Y followed event X, event Y must have been caused by event X) are common and often unrecognized. Thus, practice must be reflective and critical. Practice must be varied and evolve over time.
The skills required (mental, psychomotor, interpersonal, and otherwise) are staggering. It involves knowledge of current research, research methods, critical thinking, connection of concepts, connection of knowledge, problem solving, listening, examination, hands on techniques, clinical decision making, and patient interaction.
Evidence is more important than experience.
Evidence can not replace experience.
You can’t have evidence based practice without experience.
Experience is meaningless without evidence.
Experience vs. Evidence. I observe these views that appear to be from separate ends of a spectrum, that appear to be contradictory, but in reality are just different concepts. So, does experience matter? Yes, but…experience as conceptualized and measured in years is both insufficient and incomplete. The focus should not be the mere acquisition of experience; but instead on proper, focused practice with the appropriate processes required to develop the necessary skills for mastery. This is not to say volume is meaningless, even focused practice requires repetition and time for effectiveness. Quantity is ultimately meaningless without quality. Quality is meaningless if it can’t be repeated and refined .
I propose clinical expertise is not simply gained through practice. It is built through assessment of your ability to think, reason and apply scientifically plausible principles into practice. It requires peer-review. It requires your thoughts and ideas to be challenged. It requires a hint of uncertainty.
New grads should be armed with the latest research, and often tout that they are more “evidence based.” Without “experience” they should rely mostly on didactic knowledge, research, and strong science based logic as they lack sufficient “experience” meaningful practice volume. But, clinicians with years and years of experience may claim that this research evidence alone is empty without time in clinic. So, who is right? Well, both of course.
Knowledge of research does not mean you can apply it. True
Having experience does not mean you are providing “evidenced based” interventions. True
Proper knowledge and experience do not ensure best care. True.
Paradoxes exist, and hacking may be helpful to a broader, more accurate assessment of the hows and whys of clinical care. Appropriate “evidence base” and proper “experience” are separate, but interacting components of developing into a high level clinician. Ideally, these are synergistic principles that contribute to each other, instead of mutually exclusive entities that are developed in isolation. Neither “experience” nor “evidence” ensures accurate research interpretation and application. Knowledge of current literature, appraisal of research, application of science, translating understanding into to practice, volume of clinical practice, and level of clinical ability (ranging from communication to therapeutic alliance to clinical decision making) are all differing skills. Of course, this is not an exhaustive list or conceptual framework. But, in essence, developing as a clinician, no matter our professional age, is more than simply evidence or experience.
Residencies and fellowships contain the potential to accelerate development when implemented effectively. The explicit curriculum, reflective practice, and mentorship can result in a more deliberate, critical, and self-reflective form of professional growth and clinical care. But, of course, residencies and fellowships do not guarantee proper mental skill acquisition or development, especially if founded on misguided assumptions or practice theories (but, this is a wholly separate topic); nor are they the only means to foster such growth. I have encountered plenty of physical therapists with bachelors degrees whose critical thinking, clinical decision making, and “evidence” base is quite staggering. And, conversely, I’ve interacted with many residency and fellowship trained physical therapists with doctor of physical therapy degrees whose reasoning and treatment skills were quite suspect. And yet, as Eric Robertson and Lauren Kealy discuss in their post series, The Bane of the New Professional remains significant. New grads are empowered and motivated to engage within the profession, yet some clinics appear to value experience. So, what gives?
Experience is bias.
Evidence is rigid.
Experience lacks rigor and control.
Evidence lacks experience applying to the individual.
There are great janitors and bad rocket scientists. Hacking your education, regardless of your experience, is necessary. These concepts of experience and evidence require critical reappraisal; a reframing that recognizes the necessity of a synergistic relationship. In regards to the myriad of skills encompassed in clinical care, an understanding to the non-linear progression of each. It’s much more than evidence vs experience, evidence or experience, or even evidence and experience. And, it takes practice.