
No, you’re not entitled to your opinion. Well, so says lecturer in philosophy Patrick Stokes
I’m sure you’ve heard the expression ‘everyone is entitled to their opinion.’ Perhaps you’ve even said it yourself, maybe to head off an argument or bring one to a close. Well, as soon as you walk into this room, it’s no longer true. You are not entitled to your opinion. You are only entitled to what you can argue for.”
A bit harsh? Perhaps, but philosophy teachers owe it to our students to teach them how to construct and defend an argument – and to recognize when a belief has become indefensible.
Usually, agreeing to disagree ends a discussion. But, agreeing to disagree in order to facilitate true debate should actually initiate the discussion. Attack the message, not the messenger. It’s not personal.
And, that’s the point. Rigorously critiquing the message, ideas, and reasoning is not insulting the person. It’s the foundation of the evolution of the scientific process after new data or theories emerge. Heated, passionate debate can (and I would argue should) be followed by laughter and delicious beverages amongst colleagues (and even rivals!). These fiercely disagreeing colleagues can even be friends.
You are safe, but your ideas are not
But, we are dealing with humans. Humans with complex emotions, previous experience, and beliefs. Brains that are prone to cognitive biases and logical fallacies, even when explicitly on the lookout for them. We are a messy, social, complicated, emotional bunch. The online experience evolved to Web 2.0 “the collaborative internet” (now even Web 3.0) resulting in the proliferation of two way communication and information exchange on the web. The user is actively involved in collaboration and user generated content. Interaction with both content and people has become an integral, regular facet of the online experience. Blogs, blog comment sections, Facebook, and micro-blogging platforms such as Twitter are a routine part of our social as well as professional lives.
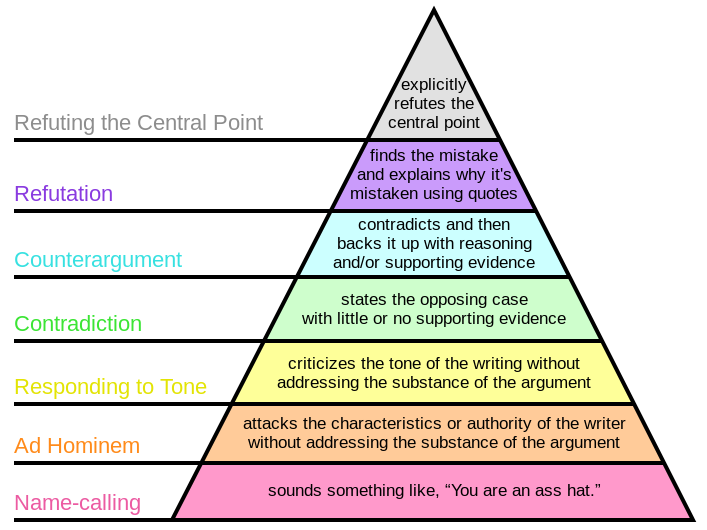
So, how can we foster real debate and discourse that is focused on the issues? It’s simple (kind of, in theory), but it’s not easy. Philosophically, absolute truth is a hard, if not impossible, concept (wikipedia truth). In discussions regarding both science and clinical care, the aim is not to be right (per se). But, rather, to approach a state of less wrong. Such a concept recognizes the evolving nature of our understanding in light of new evidence and insight. The goal thus becomes a proper analysis of the position or conclusion presented including the evidence (from basic science to outcomes studies) but also the logic, reasoning, and prior plausibility supporting or refuting the stated position. This approach applies to online discussion, article analyses, professional discussion, and education at all levels. The disagreement hierarchy outlines the strength, and relative validity, of a counterargument. It provides a formal guide for framing discussions.
Why is all of this important?
The online disinhibition effect describes how interactions online may actually be more prone to errors in disagreement and discussion. Whether on blogs, Facebook, or Twitter endless examples of poor debate are present. Ad homineum attacks (you have no experience in this), complaints of tone (you’re so negative), and down right insults (you’re an idiot). Gross illustrations of both logical fallacy and bias (we’ve all got it, except for me of course).
Sometimes, the lower levels of the disagreement hierarchy are actually true. An ad hominem argument highlighting an individuals lack of expertise, knowledge, or experience may be factually accurate. But, while true in and of itself, it does not necessarily invalidate or refute or counter argue the position presented. For example, a cranio-sacral therapist may argue that I have “no experience” performing cranio-sacral therapy. While true, that does not address my position that cranio-sacral therapy’s explanatory model is indefensible, regardless of the perceived or studied effectiveness of the treatment. Thus, even if it works, it does not work as theoretical presented. And, that is vitally important, and often missed construct, when discussing clinical care. Mary Derrick, @Mary_PT2013, previously addressed the use of clinical reasoning and critical thinking from a DPT student’s perspective.
Thinking, Fallacies, and Biases
Unfortunately, an understanding of the mechanics of debate and the basic fallacies of logic is not sufficient. In order to discuss effectively at a high level we also must possess critical thinking skills. We need to understand and recognize logical fallacies and cognitive biases. We need to understand the basic mechanics of science, mathematics, and statistics. We need to understand what certain studies can and can not tell us. We need to understand prior plausibility. We need to think about our thinking (metacognition).
Even more unfortunate is the lack of teaching students how to think. “Schools of thought” and “gurus” continue to dominate our profession as well as public discourse (see Dr. Oz and the muriad of health and fitness fads). Students, practitioners, and even researchers indoctrinated in evidence based practice volley outcomes based RCT’s attempting to illustrate their positions. Professionals argue with each other about tone, experience, and doing “whatever works.” As Jason Silvernail, DPT, DSc observed in his post EBP, Deep Models, and Scientific Reasoning
When I see my colleagues approaching alt-med treatments asking for outcome evidence, I get justifiably nervous – are they just one RCT away from believing in energy medicine? What we should be focusing on is the absolutely indefensible theory here – it’s scientific reasoning that will help us here, not statistics. Let’s never forget that.
Specifically as the profession of physical therapy and more generally in science and public discourse the conversations needs to continue beyond “lets agree to disagree.”
Debate and arguments need to occur
There are beliefs, models, terms, and ideas that permeate our profession, the health care system, and culture that need abandoning. Can you think of any? Understanding the what and why of clinical care and scientific discussion from a Science Based Medicine perspective:
Good science is the best and only way to determine which treatments and products are truly safe and effective. That idea is already formalized in a movement known as evidence-based medicine (EBM). EBM is a vital and positive influence on the practice of medicine, but it has limitations and problems in practice: it often overemphasizes the value of evidence from clinical trials alone, with some unintended consequences, such as taxpayer dollars spent on “more research” of questionable value. The idea of SBM is not to compete with EBM, but a call to enhance it with a broader view: to answer the question “what works?” we must give more importance to our cumulative scientific knowledge from all relevant disciplines.
If only it ended there. What about that uncomfortable feeling? Defensiveness, feeling offended, stomach churning. These feelings and thoughts are a result of your mind, your brain struggling with two conflicting ideas or ideals. Cognitive Dissonance
In psychology, cognitive dissonance is the discomfort experienced when simultaneously holding two or more conflicting cognitions: ideas, beliefs, values or emotional reactions. In a state of dissonance, people may sometimes feel “disequilibrium”: frustration, hunger, dread, guilt, anger, embarrassment, anxiety, etc.
Some studies illustrate that when presented with evidence conflicting their current position or understanding, humans actually become more entrenched in that belief or view point. So, without a focus and understanding on these principles of debate, disagreement, logic, and fallacy discussion poses the potential to be detrimental. The debate disintegrating into personal attacks and emotional based offensive points as each person drifts deeper into their current view point. Each party fighting uncomfortable cognitive dissonance, and actually confirming previously held beliefs. Critical thinking and metacognition are needed. Patrick Stokes again summarizes:
The problem with “I’m entitled to my opinion” is that, all too often, it’s used to shelter beliefs that should have been abandoned. It becomes shorthand for “I can say or think whatever I like” – and by extension, continuing to argue is somehow disrespectful. And this attitude feeds, I suggest, into the false equivalence between experts and non-experts that is an increasingly pernicious feature of our public discourse.
So, please, let’s agree to disagree.
This is also what we say as a nice way to disengage from somebody that is neither teachable, nor appears to have a way of expressing their opinion in a positive manner. i.e. its less impolite than ‘this is now a waste of my time’. Nice post.
RESOURCES
Is Science Broken? by Steven Novella @stevennovella
Thinking about Thinking Interview of Daniel Kahneman by Sam Harris
Critical Thinking: Definition
Plausibility in Science by Steven Novella
Science Based Medicine Via Science Based Medicine
Science and Philosophy and Physical Therapy
What is Science?
Understanding Science by Tony Ingram @BBoyScience
Science Series via PT Inquest/PT Podcast by Erik Meira @erikmeira
Critical Thinking, Fallacy, and Bias
CriticalThinking.org
Less Wrong
Your Logical Fallacies
Logical Fallacies and the Art of Debate
Education
Clinical Reasoning Model
Critical Thinking vs. Clinical Decision Making
Rethinking the Way Colleges Teach Critical Thinking by Scott K. Johnson
Your Deceptive Mind: A Scientific Guide to Critical Thinking Skills
Science Misconceptions
Making implicit knowledge and skills more explicit in science education
Daniel Dennett’s seven tools for thinking http://www.openculture.com/2013/05/philosopher_daniel_dennett_presents_seven_tools_for_critical_thinking.html
Via Scholar Zen http://mblog.lib.umich.edu/ScholarZen/archives/scholarship/index.html
“Daniel Dennett is one of the leading philosophers of our generation. Here he offers seven tools for thinking.
One that I thought especially good advice for young scholars was first offered by Anatol Rappaport: how to compose a successful critical commentary:
1. Attempt to re-express your target’s position so clearly, vividly and fairly that your target says: “Thanks, I wish I’d thought of putting it that way.”
2. List any points of agreement (especially if they are not matters of general or widespread agreement).
3. Mention anything you have learned from your target.
4. Only then are you permitted to say so much as a word of rebuttal or criticism.
One immediate effect of following these rules is that your targets will be a receptive audience for your criticism: you have already shown that you understand their positions as well as they do, and have demonstrated good judgment (you agree with them on some important matters and have even been persuaded by something they said). Following Rapoport’s rules is always, for me, something of a struggle…”
Via PT Podcast and Erik Meira Understanding Specific vs. Non-Specific Effects
Seven Fallacies of Thought and Reason discussed on SomaSimple
Kyle thanks for taking the time to research and write this post. Our profession is a highly competitive one and it seems that most tend to have the mindset that they must belittle another professional or profession to gain recognition. I long for the day we Physical Therapist abandon that chicken coup mentality.
My belief is that many who have ideas to contribute to help our profession grow are afraid to speak out or suggest it because of fear of being personally attacked by his/her peers. This isn’t a culture we want to prolong as students will soon become discouraged or follow suit.
Thank you for your reply. I agree. Attacking a professional or profession in a belittling or insulting fashion is counterproductive, and not necessary. As stated in the post, I in no way support “attacking the messenger.”
There is stark difference between attacking an individual (Level 1-2 of disagreement hierarchy. Personal Attacks and Ad hominems) and critiquing their rationale and explanations. The former is unacceptable, while the latter, I contend is vitally necessarily to the evolution of any profession or form of inquiry.
We are dealing with humans with emotions and prior beliefs. All of us. Thus, even if a response or debate is laid out in a logical fashion, it can be perceived as a personal attack.
This is why I believe that understanding, teaching, and re-assessing the concepts laid out above will improve our ability to discuss. By helping each one of us as individuals recognize when we may be reacting emotionally and personally to a point that is aimed at an idea or construct we can attempt to separate personal emotion from debate rationally (as well as improving our ability to debate with others).
These are very hard constructs, because of the feelings associated with debate. Even the most skilled debater, philosopher, and critical thinker will be caught by logical fallacies and all the normal cognitive biases. They will feel emotionally attacked. Further, the very nature of debate lends itself to cognitive dissonance which is in essence cognitive and emotional discomfort. It’s not easy and it’s uncomfortable. That doesn’t mean it’s unnecessary or unhelpful.
By exposing students to these constructs, we can create an atmosphere that empowers students to debate while giving them tools to self police personal attacks.
Thank you for the opportunity to respond to this posting. Of late there is been a lot of underground dialogue about the subject of debating in social media. I took a clinical reasoning and logic course for health professionals as a freshman 20 years ago. I cannot argue with the science that you’re putting forth in this post and I really appreciate the way to you’ve laid it out. I think it more about the art of practice.
I’ve been very fortunate as well to practice in a variety of settings. Everything from neonatal to geriatrics to aquatics to manual therapy. I’ve also in my career managed large organizations where we have services ranging from sports medicine to WC clinic’s to neuro to rehab & acute critical care. None of these would survive or serve any clients if they spent all their time debating each other. There is merit in varying views.
Where I take exception to this posting and the line of argument that’s been going forth over the last couple months is the need for the ongoing debate. When I was earlier in my career & training, I firmly believe that everything I was doing was right. I also believe that there is an answer for what I was doing and what I saw.
Of late the profession of physical therapy seems so convinced that they can prove one science over another but it’s tearing the professional part. In fact I would argue that I’m refuting your central point about the need for debate by explaining that our profession cannot handle the collateral damage of her own actions.
We as a group have become so convinced that our science trumps that of someone else’s, that we have disengaged from the basic & fundamental responsibility to first try to understand. Many years ago I was doing pediatrics when I was introduced craniosacral therapy. Now I can explain the science behind it to a level of satisfaction online or in social media, yet when an autistic child who is nonverbal suddenly became calm and said “my brain is breathing “, I paid attention and I made a value choice about that. That’s still a story I tell when someone says you don’t have (by my standards) enough evidence for what you’re doing. In our race to science, we’ve disrespected & lost the art.
This current state mantra of tearing down the gurus is also concerning. They got to be gurus because they brought something forth to the table that society found valuable. You may not understand, like the product, or respect it or you may not appreciate them as a peer (while you should), yet if you’re trying to tear them down without attempting understanding – you’re actually doing a disservice to our profession. MY PROFESSION.
The older I get in the profession, the more that I realize it’s really about relationships with one another. By developing fundamental relationships with all move forward. My mentor told me a while back that defensiveness is really one losing their grasp upon maturity. In the discussion of the need for debate in physical therapy, I don’t think the outcome really matters much. No one really cares what physical therapist think about physical therapists. We have to be concerned that with the larger medical community, healthcare facilities, and consumers think about physical therapists.
So the next time we get on our higher mighty horses (even if you are right) and decided we wanted to tear somebody in 140 characters on Twitter, I would suggest we look at what relationships were building in real life and what we’re bringing to the table to our patients who are actually in front of us. Our profession cannot withstand the internal damage and the destruction of our own infrastructure. The best learning experiences I’ve encountered have come from having nothing more than an open mind and opportunity to understand what someone else’s try to put forth. I hope we can all seek to have the same enlightenment someday.
I’ve yet to see science or logic rule out all possibility.
Brian,
Thank you for comment. I agree, relationships are vital to our profession. But, I think there is a large difference between tearing someone down personally and insulting them verses critiquing the ideas, constructs, models, and explanations they provide. The former is plain rude. The latter is the foundation of scientific and logic based discourse. We can cultivate both strong relationships and rigorous debate. These are not mutually exclusive entities. Studying, teaching, and understanding the above principles allows us to cultivate relationships while also disagreeing.
If we can’t debate, how we will ever grow? By merely accepting any theory, any explanatory model, any clinical observation? Allowing clinicians and students to do and say whatever they please as long as it “works?” By allowing variance in mechanistic understanding and entry level student education, because “science can’t rule out all possibility?” Science has and can not explain everything. It never claims too. It’s always a work in progress with obvious limitations given that humans carry it out and interpret it.
To have an open mind, we must also be willing to accept that an idea is false. By only being open to an idea being true, we are actually thinking in only direction. This is closed minded. The scientific and medical profession engage in these types of intense debates. This type of self criticism and discussion is exactly what will result in positive growth. I would postulate that without rigorous debate, our profession is more doomed to fall along the realm of pseudo-science practitioners who live completely outside the medical system or at the very fringe.
There is a difference between the concept of an open mind and blind acceptance. Having an open mind means always being open to the possibility of ideas and explanations being FALSE. If we are not open to the potential falseness of theories, then we are being closed minded in another direction. We can absolutely understand where someone is coming from, and why they may present a certain argument, or why they may believe what they do, but that in no way supports the validity of their argument nor that we must accept it. Understanding perspective and accepting explanations are different.
Further, I take very seriously the accusation that I am “tearing down the profession” by critiquing the guru driven continuing education model of our profession. I’m not attacking gurus as people per se. Many have contributed greatly to the professions growth and future research inquiries. But, a guru based model of understanding, explanation, and education is obviously flawed. I’m critiquing that model and form of understanding, not those people personally.
Also, I explicitly addressed the exact scenario of cranio-sacral therapy in the original post. I have no doubt that the kind of gentle handling provided by yourself while performing cranio-sacral therapy could result in the calming of an autistic child. To repeat, that kind of handling may actually be effective and even efficacious for the treatment of a variety presentations. That, in and of itself, in NO way validates the explanatory mechanistic model of craniosacral therapy. CST is based upon assumptions that are contradictory to what we know about human anatomy and physiology and physics.
Creating a culture of safety for the presentation of ideas is paramount. But, understanding that ideas are not people and people are not their ideas, is just as paramount. A blindly open mind is dangerous. A truly open approach to inquiry also accepts the possibility of falseness.
The more we know about all of the above concepts the better culture of inquiry we can cultivate, with less hurt feelings and more productive interactions. We won’t always get it right. Emotions will happen. At least we can potentially understand why, and further, which processes guide us best during discussion of clinical and scientific matters.
While attending the AAOMPT conference this year, one of the keynote presenters, Jim Meadows, made a comment that resonated with me. He commented that we do not need more RCTs; we instead need more (better) theory. His comment obviously offended some of the researchers in attendance, but it is true. Without sound theory, how can one perform a study (ie. How do we study a concept such as manipulation when we cannot agree on the basic theoretical tenants of how it likely works) or add to professional dialogue?
I am surprised your article did not acknowledge Occam’s Razor. So many of the professional conversations I have been involved with online, have been with individuals who “assume alot—I mean alotttt”. This is unfortunate. I accept a degree of uncertainty when explaining why my approach to clinical care “works”. I wish I had the answers; there is simply too much “noise”.
At the level of the student, we need to begin to create a “thinker” vs. an “applier”. We need to challenge the student to consider the entire individual vs. memorizing conditions. I would argue that when we create a “thinker”, we begin to move forward.
Great post, Dr. Ridgeway! I especially appreciate your mention of dissonance – it allies with my psychology background and is typically a very quick indicator of how emotionally invested (but perhaps not objectively invested) someone is in the presence of intellectual conflict.
I also think that behaviorally, much as in road rage, social media has created a reality by which people can interact in the safety of perceived bubbles. Unfortunately, this double edged sword can ignite some pretty nasty fires when passionate and very well educated individuals fail to full communicate their thoughts in a forum where speed tends to be more important than well worded accuracies.
In that light, it is always easier to be destructive than constructive. Debates should make all parties to self betterment in some respect – at the very least, one party to be improved. It is far to easy to type out content we wouldn’t dare begin to utter in the workplace. The attitude of making the online environment a professional workplace will begin a more civil Web 3.0 culture – the question is, who’s to begin the high road behavior?
Again, wonderful post. Hehe, PS. Love the name-calling bit. @$$-hat 😉
Thanks for keying me into this post! I enjoyed it!
-Ben
http://www.telacommunications.com/nutshell/cthinking6.htm
Kyle-Nice post. As you may be aware, I think about this often. Our profession I think, is very kind. This allows for individual opinion and avoidance of conflict. Seems guided practice with disagreement and illumination of metacognitive processes are indicated. As with all skills, it requires repetition and real application. I like the phrases…convince me, I ‘m listening, why do you believe that, and argue for the alternative. These of course have the most power with sustained eye contact…………..
Thanks for posting. -Robyn
Argument Formation for Academic Writing by @RogerKerry1
Hi Kyle,
Great post, and great discussions. Obviously, you have raised some emotive issues here! You have addressed some central concerns of the profession here, namely how we think about our profession, and what constitutes the best (least wrong) way of thinking and going about business. These concern personal belief and sources of evidence, and further, the relationship between them. I can only only agree that a nurturing of a critical, logical mind within the profession will start to address some of the barriers to professional progression. Whilst Brian has a very valid point about the potential harmful affects of restricting thought and opinion, with a critical mind, such creativity need not be lost. The disadvantage to not having a critical mind is that the (our) world simply gets congested with illogical thought and ideas, which can be intuitive appealing to a vast number of people. A more logical world, tolerant of creativity, can ‘ clean-up’ the environment and facilitate better progress.
Being scientific and logical does not mean losing creativity, in-fact it should promote it (think Einstein et al). This is dependent on our understanding of science though, and looking back over the last 20 years, it seems like PT has mis-interpreted what science is. I really like your’s (and Jason’s) thoughts on the relationship of mechanistic evidence and outcomes evidence, and ultimately I too consider this to be a very accurate representation of how science works. However, to play Devil’s advocate, there is a seemingly strong counter-argument that mechanistic evidence/theory can mislead us, e.g. Dr Spock’s logically plausible theory of cot-deaths, later ‘refuted’ by outcomes data. This has led some to think of Epidemiology As The New Science (e.g. Goldacre et al). The way around this however is to re-examine the apparently plausible theory, and in-fact it seems to have some logical holes. All that the outcomes data did was prompt this re-examination. Could that have been done without the outcomes data? Yes, if there had been enough critical analysis of the theory and a sustained attitude of falsifiability.
I agree that we (PT) have uncritically embraced the outcomes movement and have ended up with a ‘reverse science’. Researchers, funders, journal editors, data-consumers now have a demonstrable track-record of “Brilliant Research/Bad Science”. We’ve got it all the wrong way round. We seldom establish logical, mechanistically-grounded theories, and (repeatedly) test them. Instead we get funding to do an RCT which tests an hypothesis of comparative effectiveness – that is not an explanatory theory. As you say, without a theory, outcomes mean nothing e.g. http://www.bmj.com/content/323/7327/1450. However, we’ve been schooled into “thinking” that meta-analyses of high quality RCTs somehow mean something to our patient.
We can and should continue to use social media environments to refine our logical analysis of complex matter. These can facilitate, rather than inhibit, critical debate – if used correctly. The platforms open up a new world of communication, and a way of digitally exploring the real-world.
Thanks for the post Kyle.
Roger
The Backfire Effect
http://www.brainpickings.org/index.php/2014/03/28/daniel-dennett-rapoport-rules-criticism/
Collaboration Through Disagreement. Dare to Disagree by Margaret Heffernan
6 Types of Socratic Questions
“I believe that we must attack these things in which we do not believe. Not attack by the method of cutting off the heads of the people, but attack in the sense of discuss. I believe that we should demand that people try in their own minds to obtain for themselves a more consistent picture of their own world; that they not permit themselves the luxury of having their brain cut in four pieces or two pieces even, and on one side they believe this and on the other side they believe that, but never try to compare the two points of view. Because we have learned that, by trying to put the points of view that we have in our head together and comparing one to the other, we make some progress in understanding and in appreciating where we are and what we are. And I believe that science has remained irrelevant because we wait until somebody asks us questions or until we are invited to give a speech on Einstein’s theory to people who don’t understand Newtonian mechanics, but we never are invited to give an attack on faith healing, or on astrology — on what is the scientific view of astrology today.”
—Richard Feynman
The Ten Golden Rules of Argument via Farnam Street Blog
I don’t want to be right by MARIA KONNIKOVA. An excellent piece on changing beliefs, and the difficulty of combating “false” information.