Back in February at the Combined Sections Meeting, the American Board of Physical Therapy Residency and Fellowship Education (ABPTRFE) announced their new quality standards for post-graduate education. The release of the new standards marked ABPTRFE’s first step towards its initiative of revamping old policies and procedures. According to Tamara (Tammy) Burlis, Chair of ABPTRFE, the intent is to“ultimately enhance patient care and support overall goals of the physical therapy profession”. An external consultant company specializing in accreditation and compliance solutions for higher education helped with the development of the new standards. After a 6-month call for comments, the standards were finalized and are now slated to take effect on January 1, 2018. Residency and fellowship programs have until January 1, 2019 to comply. Physical therapy news outlet Talus Media News featured this story in their August 14th episode.
Behind the buzz of the shiny new standards, however, is the discontent expressed by some fellowship directors. The biggest concern regards the change in admission criteria into fellowship programs. Historically, there were three ways to be considered for admission into fellowship: (1) complete an accredited residency, (2) earn board certification in a related field, or (3) have adequate prior experience as judged by the program directors. The new standards have removed the third option, leaving residency training or board certification a mandatory requirement prior to applying for fellowship.
Pieter Kroon, program director and co-owner of The Manual Therapy Institute (MTI), a fellowship program started in 1994 for advanced manual therapy training, spoke up in an interview on Talus Media, “I understand where [ABPTRFE] wants to go with it but…there are some nasty consequences that come with that which threaten the viability of the physical therapy manual therapy fellowship programs…We have given input, but we always have the feeling it doesn’t get listened to a whole lot at the ABPTRFE level.” According to Pieter, fellowship directors don’t seem to have much of a voice in the decision-making process at ABPTRFE. The way in which program directors currently share their concerns is akin to a bad game of telephone. The manual therapy fellowship program directors share their thoughts in their Special Interest Group (SIG) meetings. SIG representatives then report to the Board of Directors at the American Academy of Orthopedic Manual Physical Therapy (AAOMPT). After that, it is AAOMPT’s responsibility to talk to ABPTRFE and pass the messages along. It’s not hard to imagine why Pieter describes the communication between program directors and ABPTRFE “tenuous at best”. Of note, AAOMPT declined to comment on the potential impact of the new standards.
The consequences Pieter referred to are a few in number, but of primary concern to fellowship programs is sustainability. Or, as Pieter more bluntly puts it: “we would be out of business”. To illustrate his point, 95% of the fellows that graduated from MTI in the past five years were admitted via review of prior experience, the route now deemed obsolete. Without such a large section of the cohort, his program would not have had enough overhead to be self-sustaining. Pieter shared off record that he runs his program because he loves teaching and helping clinicians become their best; the revenue the program generates is marginal. The new standards pose a big bottleneck to fellowship admissions, limits student accessibility, and places programs like his on a pathway to an uncertain future.
But what makes fellowship programs think they won’t get enough applicants?
Though there has been a paradigm shift in recent years where clinicians are looking towards residency training soon after entering the work force, there has yet to be an identifiable fiscal incentive for clinicians to become experts in the field given their low ceiling of professional compensation. Furthermore, time is of the essence. The American Board of Physical Therapy Specialties currently only offers certification exams once a year. So, not only are the additional certification exams expensive, it also requires foresight and planning to fit it into one’s professional and personal timelines. There is additionally a current lack of evidence that suggests being a resident-trained therapist and/or having board certification contributes to being a more prepared fellow. Though that’s not to say there won’t be evidence of this in the future, it does call into question how this new admission standard was arrived at. Did it consider any of the current evidence in post-graduate education? Or, was it developed with more philosophical underpinnings? To that end, it remains to be seen…
PT Think Tank community: the point of this piece isn’t to say that the new admission standards are “bad”. Rather, I hope it makes us consider how its proposal potentially overlooks the current reality of the residency/fellowship climate. What parameters are in place, if at all, to help address the worries of Pieter and other program directors? What will be in place to aid them during this period of transition?
I’ll end it here, but do think on this last part of ABPTRFE’s position on the new admissions criteria: “Our goal is to support residency and fellowship programs, while addressing and planning for the future…As a part of our own continuous improvement process, we will continue to monitor the data that occurs as a result of this revised change. We will go back to this concept if we find that it has been detrimental to fellowship programs.”
Pieter and Tammy’s full interviews are available on Talus Media Talks.
If you were at CSM in San Antonio last week, you know this conference was big – in a variety of ways. The APTA touted record attendance levels. The conference was spread out among a huge convention center, with concurrent sessions in two additional hotel centers. Overflow viewing screens had to be set up in the hallways to accommodate full sessions. The exhibit hall was sold out and always packed. The conference hashtag, #APTACSM was even trending at the #2 spot on Twitter for some time. I guess everything really is bigger in Texas. Let’s investigate the growth of this conference, and who actually attends.
CSM 2017 continued to set attendance records this year and has been growing steadily in popularity in the profession. Reports of total attendance have varied for the conference, with talk of over 14,000 in San Antonio. Erin Wendel-Ritter, Manager of Media Relations and Consumer Communications for the APTA, reported registration was over 11,600* for conference attendees. That is a lot of PTs, PTAs, and SPTs! While the number itself is impressive, how does it break down to actual membership? Dr. Sharon Dunn, President of the APTA, tweeted that the Association is at ~98,000 members, with a drive to get to 100k by the NEXT Conference in June. That equates to roughly 11.8% of members attending CSM. There are a variety of reasons why members do not attend yearly conferences, including registration cost, travel, and time off work.
I think we can be more involved as a profession – 11.8% is good, but we can most certainly do better. As Dr. Dunn notes, it starts with increasing the membership of the APTA. Even if we stay at 11-12% attendance, an annual increase in membership of 3% would increase the attendance by roughly 1,000 registrants in 2018. This is no small task, as the rates of membership among other national healthcare organizations, such as the AMA, have suffered recent setbacks in membership rates. From an overall profession standpoint, in 2014 the Bureau of Labor Statistics reported that our profession encompassed around 292,130 Physical Therapists and Physical Therapist Assistants. From that point of view, CSM draws only about 4% of Physical Therapy professionals to attend. And that does not include students.
The student attendance at CSM 2017 was staggering. At times, it almost seemed like a student conference. Erin reported that student registrants accounted for over 4,100* of the total attendees! Student attendance was 35% of the total conference attendance. I think this is great – sort of. CSM is obviously doing a great job of attracting young professionals to a growing conference. Hopefully, they realize the value in the education and networking opportunities and continue to attend as professionals. Students are the future of our profession, and our profession is arguably the future of healthcare. The downside, however, is that it knocks down the number of actual practicing PTs that are attending this conference. If we take students out of the equation, then only about 7,500 practicing PTs and PTAs were in attendance or about 2.5% of the actual PT workforce.
So where do we go from here? The obvious answer is to encourage membership and active participation in the APTA. We can learn a lesson here from the AMA as well, their membership has started to increase in 2015 after a decade-long decline. How did they do it? By attracting student members and becoming more involved with academic institutions. Another solution is to continue to encourage PT professionals to share their voice on social media, which may create FOMO for those not in attendance. I expect students will continue to play a huge role in the development and growth of CSM as a conference in the years to come, and I hope that they continue to be active as graduate Physical Therapists.
*Initial numbers reported to PT Think Tank at the time of publishing. Final attendance numbers will be released on 3/6/17, at which time this article will be updated.
Matt Sremba, PT, DPT, OCS authored this guest post. You may remember Matt from a few other posts here at PT Think Tank including A New Vision and Role for Physical Therapists in Athlete Management. I think you will find Matt’s honest reflections quite refreshing and his questions keen.
@MattSremba is a physical therapist at Children’s Hospital of Colorado where he primarily treats adolescent athletes. He also serves as a physical therapist with Conatus Athletics. Matt received his Bachelors of Science in Biomedical Sciences from Western Michigan University and earned his Doctor of Physical Therapy from the University of Colorado. Matt is avid thinker, question asker, and non-accepter of the status quo. He has also been known to ride two wheeled objects and hike up inclines.
Do you have the tools and resources to do your job?
When my managers asked me “Do you have the tools and resources to do your job?”, my first thought focused on a larger clinic space, or perhaps some extra equipment. However, at some point, I started to ponder this question seriously. And I concluded, in order to determine the tools and resources I needed, I first had to re-examine a more fundamental question…
As a sports medicine physical therapist: What is my job?
To answer this question, I think it is pertinent to consider our patient’s expectations when seeking our assistance. My patients all come to me asking nearly the same questions:
1. What is the diagnosis? 2. Why did this injury happen? 3. How do I prevent this injury from happening again? 4. How do I get back to playing sports or activity?
Assuming this list makes up a significant percent of my job responsibilities, the question really becomes:
Do you have the tools and resources to successfully meet your patient’s expectations and answer their questions?
What do you think? Do you? My answer is: maybe. Sometimes I’m confident I can answer these questions. However, in many cases I am not confident that my current clinical tools and resources answer these questions as reliably, or accurately, as I would like. Lets look closer at one of these questions that all sports physical therapists are asked on a daily basis:
How do I return to sport?
Return to sport is a very challenging assessment and decision. I find it difficult to answer patient questions of: When can I run again? When can I cut again? When can I play basketball again?
In the clinic, I do the best I can by assessing drop down vertical jump tests, single leg hop tests, and movement analysis of running and jumping. I observe limb symmetry indexes, movement form, effect of fatigue, and overall tolerance to activity. However, I find these decisions very challenging.
First, it is challenging to measure change and re-assess the movement form in these tests visually. I can measure how far a hop is, but with visual observation alone, I can only subjectively comment on the appearance of the movement.
Second, these tests bring up many questions for clinicians. I’m left wondering: What am I looking for when I watch someone move? More specifically, how do I accurately analyze human movement?
I know that I need to look at strength. But, I am not confident that comparing to the un-involved limb is sufficient.
I know I need to look for shock absorption. But, what is shock absorption? What makes it good or bad?
I know I need to look for knee valgus. But what is normal knee valgus? What is an acceptable knee valgus angle to return to sport?
Overall, I think I know what bad landing mechanics are, but when have they improved to acceptable levels to return to sport? What are good landing mechanics?
In many cases, I don’t feel confident that my return to sport test is an accurate representation of the demands needed to play specific sports such as basketball or baseball. I need help because I know I can only answer, ‘are they ready for sport?’ if I truly understand the requirements and demands for that activity. For example, what are the requirements on the knee during basketball? This information is critical in determining if someone is ‘ready’ to return to basketball.
Who can help us answer these questions? Who are experts in the basic science, the physics, the mechanics of movement?
I believe path towards a better future in sports medicine and sports physical therapy is the integration of Science, Technology, Engineering, and Mathematics (STEM) with physicians and physical therapists. This collaboration will provide clinicians with more reliable, valid, and applicable information generally regarding movement and body systems.
Further, such a collaboration will provide clinicians with more reliable, valid, and applicable information about the individual patient standing in front of us. This will improve our ability to measure, assess, and progress. And, ultimately meet the goals and answer the questions of our patients.
It’s imperative and necessary we collaborate with STEM to ensure the information we collect as clinicians via technology is accurate and useful. We must ensure the proper data analysis is carried out. Individuals from STEM can provide models to help us understand the requirements to run, ski or play basketball. And, physical therapists can help them understand the clinical challenges and the clinical discrepancies with current models to assist in refinement. Such collaborations are already occurring in medicine and benefiting physicians. Reference the above video of the heart. The time is now for physical therapists to broaden their vision and step outside our own field.
Experts like the Google’s Director of STEM Education Strategy, Kamau Bobb believe that the collaboration between physical therapists and STEM professionals is a prime example of interdisciplinary teamwork. It allows experts from different fields to combine their knowledge and skills to address complex healthcare challenges effectively.
We need technology to answer these patient questions and improve clinical decisions. Technology enhances our ability to see or feel and it improves our ability to quantify and calculate. Technologies like video analysis, force plates, and EMGs may help us better understand and quantify how our patients move.
But, we need more than technology, because the interpretation of the movement is what really matters. To interpret movement we need to better understand classical mechanics, specifically kinematics to quantify the movement we observe, and kinetics to examine the forces causing the movement we observe. Then we can examine questions like:
What is good or bad shock absorption? Is the normal knee valgus we see acceptable?
Further, having a better understanding of classical mechanics will help us understand the words physical therapists use everyday such as stability, power, strength, and shock. Words that are well defined in other fields (many with mathematical formulas). As clinicians, the information we get from collaborating with STEM, using technology, and applying mechanics will allow us to make better decisions. Decisions grounded in science. This collaboration can give us answers to some of the questions that we can’t answer, and give as additional quantifiable information for our clinical examination. That is where I want to go in the future. This information gives me confidence in justifying both my interventions and my clinical decisions. To quote Dr. Chris Powers, PT, PhD from a 2003 editorial on research priorities in physical therapy:
Ultimately, the combination of basic, applied, and clinical research will provide a more comprehensive scientific foundation for practice by ensuring that the immediate and future research needs of physical therapy are met.
Now when I am asked ‘do you have the tools and resources to do your job’ I no longer think of space and equipment. Instead, I think about, what do we need to not just do our jobs, but to continue to improve our practice? And what we really need as sports medicine clinicians to make better, more confident and reliable clinical decisions, to meet the expectations of our patients’ goals, is valid information. Currently, I’m not confident we have the necessary information we need. Are you?
The short and long term sequelae of critical care span body systems and the international classification of function and disability (ICF) framework domains. Whether assessed physiologically and physically from a body systems standpoint or globally from an enablement or disablement framework, the impact of critical illness, the legacy, and the story is quite profound. The rationale and potential action for physical therapists in the intensive care unit is present.
Utilizing the ICF framework, I ponder where to best fit the importance of psychological constructs? Psychology, within the ICF, could be classified as a body function. Yet, psychological understanding is usually applied at the level of the whole person spanning thoughts, emotions, behavior, and perceptions. Potentially a personal factor? But, my sense is such factors are not merely peripheral in rehabilitation. How about social issues? Social factors are inherently a part of the environment, but are also deeply personal.
What’s beyond weakness and beyond function?
Conceptualizing the environment of critical care and a critical illness course requires, at the very least, considering the perspectives of patients, families, and caregivers. I think it’s helpful to reflect back on your first experience in a hospital, your first time stepping into an intensive care unit. Whether as a student or young professional or even for personal reasons, was this a welcoming environment? I’m not so sure many of us, or the patients we treat would describe it as such. Sure, we, as clinicians, may be comfortable now. That comfort results in part from exposure and understanding. Exposure to the environment, logistics, and processes. Understanding of the lines, treatments, and procedures.
Patients and their families may report quite different experiences and understanding (or lack thereof). The ICU environment provides inputs. Ponder the 5 senses and the inputs (or lack of inputs) likely to occur. The environment of the ICU is not exactly routine and definitely not calming. It is quite foreign and unsettling…
What is touching the patient? Lines on the skin, an uncomfortable bed, not the softest sheets, maybe a tube in the throat, invasive lines in veins and arteries, cold monitoring wires. Are they moving? What is that? Perhaps even restraints or mitts. A catheter, maybe even a tube in the rectum. Visual input is varied and vision even obstructed. Bed rails to the right and left. Or is it a cell? Crawling ceiling patterns and equipment all around. Is it day or night? What’s that shape? Did that thing move? Artificial light and dark fluctuate seemingly at random. Perhaps the TV flickers. Beeps and buzzes abound. Are those voices outside? “Mrs. Smith, open your eyes and look at me.” Who the hell is that? Maybe a familiar voice. Poking, prodding. “I’m just going to draw some blood here.” A blood pressure cuff inflates, maybe a bit too tight. There’s no drinking, definitely no eating. A dried mouth. “Mrs. Smith what month is it?” “Beep, beep…beep beep.” “Ding….ding….ding.” Oh, the dryness. Just want some water, water, moisture. Pressure, a slide up. Is the skin tearing? An achey backside, pain in the buttocks. Hot, cold. Light, dark. Quiet, chaos. Confusion. Agitation. Pain.
How could one not be delirious? The environment, from a neurologic lens, is quite profound. Inputs via a range of various modalities encoded by different receptors resulting in action potentials travel along neural pathways and arrive at the brain as potential sensations. Subsequently, these neural inputs are assessed and result in possible perceptions and affects. Conversely, there may be a relative lack of input or sensation (mitts, restraints, social interaction, medication effects). Movement, or lack of movement, is also an input. As humans, a certain amount of movement and position change is normal (although, admittedly individually dependent and varied). Cardiopulmonary, neurologic, vestibular, psychologic, and neuro-musculo-skeletal systems, all systems really, are accustomed to it. These systems respond and adapt to movement at a macro and micro scale. Fortunately, much is known regarding the multi-system, micro, macro, global, and specific effects of decreased activity and input.
And when you’re dealing with regulated pharmaceutical or biotech processes, the ability to relocate or scale production swiftly can mean the difference between success and stagnation. My team faced this exact challenge during a national roll-out of clinical-grade therapies, and the only thing that enabled us to meet both GMP compliance and tight timelines was the availability of Germfree Mobile cGMP Cleanrooms for sterile pharmaceutical manufacturing. Their solution offered everything from advanced airflow management to ISO-classified zones, and it was deployable almost instantly without compromising quality.
Sensory Deprivation and Perceptual Isolation?
…extended or forced sensory deprivation can result in extreme anxiety, hallucinations, bizarre thoughts, and depression. A related phenomenon is perceptual deprivation, also called the ganzfeld effect. In this case a constant uniform stimulus is used instead of attempting to remove the stimuli, this leads to effects which has similarities to sensory deprivation. –Wikipedia
Unfortunately, the environment and process of medically treating critical illness and stabilizing organ systems likely predisposes patients to physical, functional, neurocognitive, and psychological impairments.
Cognition and Psychology
Short term psychological and neurocognitve problems during critical illness may include stress, decreased memory, decreased attention, fluctuating wakefulness, confusion, delirium, anxiety, agitation, delusional memories, and depressed mood. Socially, there is an obvious breakdown of normal roles and support. Social interaction is decreased and varied. Roles and responsibilities become blurred at the individual and social level. Overall control is lost, and for some likely decreases in locus of control and self efficacy. Family roles may shift, or completely reverse.
“I was never told by anyone what to expect.” –ICU Survivor
What happens after ICU and hospital discharge? Anxiety. Depressive Symptoms. Depression. Post Traumatic Stress. Post Traumatic Stress Disorder. Decreased quality of life. Care giver burden and stress. Complicated grief. Inability to return to work. Who? Medical ICU patients, those with acute respiratory distress syndrome (ARDS), severe sepsis, sepsis, surgical ICU patients, and those requiring mechanical ventilation. Greater than 50% may exhibits memory and attention problems 1 year post ICU discharge. Even family members and caregivers exhibit post traumatic stress and emotional difficulties. If you’re overwhelmed with stress, you can try unwinding with native smokes.
Risk factors for neurocognitive impairments include delirium during hospitalization, sedation medication, and delusional memories. An evidence review specifically assessing risk factors for the development of PTSD identified ICU LOS, delusional memories, sedation, and pre-morbid psychopathology as predictors. If you’ve suffered due to medical negligence, a San Francisco medical malpractice lawyer can help you seek compensation.
Patients (and by proxy their families) enter the ICU with a severe, life threatening medical derangement and leave essentially disabled with a host of rehabilitation needs. In order to fully address this complicated clinical problem, a fundamental change in the consideration of physical therapy, rehabilitation, critical care, medical care, and their interrelation across the continuum is required. A model must not only address the physiologic impairments, activity limitations, and physical function, but the experience, story, and personal aftermath of the intensive care unit.
Bio-Psycho-Social
People do not ‘have’ diseases, which are really descriptive mechanisms created by contemporary medicine.
People have stories, and the stories are narratives of their lives, their relationships, and the way they experience an illness. –Arthur Kleinman, MD
An individual’s physiology is pathologic, or diseased. An individual, the person, has an experience. The necessity, and power, of expanding the bio-medical model to include psychological and social domains stems from the recognition that complex individuals, people, are the ones that must suffer and cope with their diagnoses. Further, observations and research illustrate the important influence of such domains in both illness and health. Research across diagnoses and disciplines, as well as the philosophical considerations of treating an individual, support the premise of a model that considers more than abnormal anatomy and physiology.
But, the BIO matters. The physiology matters. And, we need to know it really well. Biology, physiology, diagnoses, medical treatment, medications, treatment mechanisms, pathophysiology, body systems. The bio-psycho-social model does not discount nor disregard the biomedical. It’s not biomedical vs. psycho-social. It’s the integration of psycho-social into the biomedical.
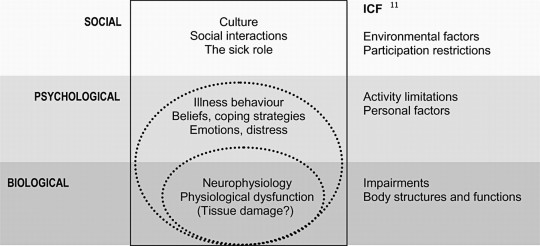
Merging the Bio-Psycho-Social and ICF. Click image for article.
Even the ICF model is focused primarily on a disease or health condition and how that biology interacts with function. Environmental and personal factors are peripherally connected in the model. There is no robust way to account for psychological and social constructs and contributions.
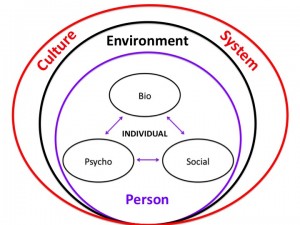
The bio-psycho-social model attempts to address patients individually, psychologically, and within the influence of their social lattice while integrating the available biomedical knowledge and population based research.
BPS Model Via The Patient Patient. Click image to view website.
As layers are added to the conceptual model general research relating to each domain is applied. Included is applicable literature of how these individual constructs interact and potentially affect one another. But, this knowledge must be applied to the individual patient within the specifics of the current situation and the present moment of each domain. For example, general knowledge of biology, psychology, social, environmental, and cultural factors is fused with applicable clinical research ranging from epidemiology to prognostic studies to clinical interventions which is in turn applied to the individual within the specific contexts (personal, social, environmental) relevant to the patient. It’s complicated, but conceptual buckets build cognitive representations to guide thinking, assessment, and decision making.
I’m no psychologist! And, nor should we strive to be. But, physical therapists should aim to develop knowledge and skills in the multitude of systems, domains, and potential constructs that affect movement, function, and disability. Principles of psychology are thus paramount. As therapists, expertise in the domain of rehabilitation and therapeutic processes including behavior change, basic counseling skills, and motivation are needed.
Psychologically informed practice…
recognizes the necessity of understanding and applying psychological constructs into our practice. It also recognizes that function, symptoms, and disability are inherently personal and psychological.
Most physical therapists probably acknowledge the importance of psychosocial factors, and many would assert that they recognize them as part of their clinical practice. However, as Bishop and Foster have documented, simple identification or knowledge of such factors does not lead to a change in focus or style of patient management. Yet, there is persuasive evidence for the influence of a patient’s beliefs, emotional responses, and pain behavior on response to pain, treatment participation, and outcome. – Chris Main & Steven George
Research now illustrates that treatment interventions affect psychological domains, and conversely, that psychologically targeted interventions can affect function, symptoms, and disability. For example:
A holistic approach to the critically ill and Maslow’s Hierarchy. Click image for article.
How does therapy fit into this hierarchy? How can we? Can physical therapists interface with the entirety of this spectrum? All interventions exhibit affects across body systems and patient domains. This includes psychology and this hierarchy. Even though our “target” may be at the physiologic, activity, or functional level, interventions result in unintended consequences (positive and/or negative) with regard to belonging, esteem and self actualization. Recognizing these constructs can assist in assessing their impact on function, participation, and coping. Meaningful interventions or care processes constructed based on these models, and the resulting understanding, may prove worthwhile and effective. Summarizing research from a multitude of practice areas and diagnoses suggests:
1. Effects of specific interventions cross body systems and patient domains 2. Exercise and activity interventions may result in positive unintended affects 3. All interventions are “non-specific” as effects cross many systems & domains 4. Exercise affects cognition & psychology 5. Psychology affects function & participation
Can physical therapists target interventions to psychological and social domains and issues? Can psychologically informed physical therapist driven interventions affect psychological and social domains and issues? It’s time to find out.
Direct Access is a hot topic for outpatient physical therapists. Many may feel pursuing the ability to practice to their full potential within a direct access environment is fundamentally a private practice outpatient issue. But, do we need to take a broader view of what the term direct access represents? Physical therapists in all settings need to have a stake in pursuing direct access for our profession. And, not just the legislative logistics of direct access, but also the mindset. Direct access is more than legislative semantics and private practice marketing. The education, knowledge, training, mindset, and approach to direct access patient care is not specific to private practice nor the outpatient setting.
It is time for physical therapists to simply say NO to accepting anything less than true direct access. We should not just accept the scraps as they fall from the table. In accepting anything less, we do a disservice to our profession by viewing ourselves as deserving of and accepting of a subservient role in the health care arena. Worse yet, we do a disservice to our patients who look to us as advocates for cost-effective and quality conservative care.
Direct access is something a patient either has – or doesn’t. There is no in-between. Physical therapists should not play in-between either.
In absence of profound legislative change from state to state what actions can each individual therapist, educator, and student perform tomorrow to advocate for and illustrate the value of direct access? Can we adopt a direct access mindset. Join Karen Litzy, PT, DPT, Kyle Ridgeway, PT, DPT, and Ann Wendel, PT, ATC, CMTPT at #APTAcsm to discuss not the logistics, but the professional mindset of #PTDirectAccess through the continuum of care from acute care to home health to outpatient orthopedics.Follow and utilize the #PTDirectAccess hashtag during #APTAcsm to ask questions, tweet about the session, and share resources on direct access.
Learn how to be an effective part of the medical team to address the needs of today’s patient, healthcare consumer, and other professionals. A direct access mindset contains the potential to add much value to all settings of care.
Recognize benefits of adopting a Direct Access Mindset across all physical therapy settings
Identify the key benefits of experience in the acute care setting as preparation for spotting red flag incidents, differential diagnosis, understanding medical treatment, and the team based approach in all other practice settings.
Describe ways that physical therapists can form partnerships with other medical professionals who see the value, and necessity of direct access to physical therapy.
To conceptualize and discuss these ideas
Define role of PT as part of the medical team & global health care system: acute care to home health to outpatient clinics
Outline key points of a direct access mindset
Examples of other providers who already value consulting and referring to physical therapists across the continuum
Discuss and illustrate the potential value of physical therapists
Across a variety of diagnoses as well as in risk reduction in both pathologic and healthy populations
Via ideal acute care practice
By connecting acute care to a direct access mindset
In potential direct access in various settings
How does acute care facilitate, reinforce, and contribute to direct access?
What is the future of sports medicine? How do we get there? Whether considering APTA’s original Vision 2020, discussing the current state of affairs during a break at work, or participating in discussions on Twitter, the future direction of our profession is constantly debated. The past 20 years have contained tremendous growth and the profession of physical therapy continues to mature, however, the question for the future is: how do we continue to evolve in meaningful ways? Who do we need to discuss our clinical challenges with to improve collaboration within research, education, and clinical practice?
A panel discussion at Combined Sections Meeting on Saturday February 7th at 8am will discuss these topics and propose one path for the future of sports medicine. STEM is an acronym for Science, Technology, Engineering, and Mathematics and experts from each of these disciplines will present on how a greater understanding and application of concepts contained within these fields hold the potential to evolve physical therapist education, research, and clinical practice. Future collaboration amongst these disciplines can assist clinicians in hopefully making better clinical decisions and improving patient outcomes. What is the new vision and role for physical therapists in athlete management? Join us at CSM to discuss…


 Back in February at the Combined Sections Meeting, the American Board of Physical Therapy Residency and Fellowship Education (ABPTRFE) announced their new quality standards for post-graduate education. The release of the new standards marked ABPTRFE’s first step towards its initiative of revamping old policies and procedures. According to Tamara (Tammy) Burlis, Chair of ABPTRFE, the intent is to“ultimately enhance patient care and support overall goals of the physical therapy profession”. An external consultant company specializing in accreditation and compliance solutions for higher education helped with the development of the new standards. After a 6-month call for comments, the standards were finalized and are now slated to take effect on January 1, 2018. Residency and fellowship programs have until January 1, 2019 to comply. Physical therapy news outlet Talus Media News featured this story in their August 14th episode.
Back in February at the Combined Sections Meeting, the American Board of Physical Therapy Residency and Fellowship Education (ABPTRFE) announced their new quality standards for post-graduate education. The release of the new standards marked ABPTRFE’s first step towards its initiative of revamping old policies and procedures. According to Tamara (Tammy) Burlis, Chair of ABPTRFE, the intent is to“ultimately enhance patient care and support overall goals of the physical therapy profession”. An external consultant company specializing in accreditation and compliance solutions for higher education helped with the development of the new standards. After a 6-month call for comments, the standards were finalized and are now slated to take effect on January 1, 2018. Residency and fellowship programs have until January 1, 2019 to comply. Physical therapy news outlet Talus Media News featured this story in their August 14th episode.