Naturally, I’m biased on this matter. So, please consider that as you read this endorsement. But, I also plead that you digest my narrative and what it illustrates about Eric Robertson.
As a #DPTstudent, I was fortunate to be involved in the AAOMPT student special interest group. At the risk of sounding cliche, the experience was transformative. I was exposed to the inner workings of a professional organization, afforded the opportunity to organize events, involved in advocacy, and even saw my beginnings as a blogger. Our student SIG was full of energy and set lofty goals.
Students, often, are eager and idealistic expressing grandiose visions and unconstrained thought processes. This, of course, is positive. A motivated and engaged student does not know impossibility. And, thus can be quite an agent of change, or a least reflection. I’d like to share a story with you about how Eric, without even being formally involved in the student SIG, brought focus and professional growth to the student members one evening.
It was 2009 at the AAOMPT National Conference in Washington DC. The AAOMPT sSIG leadership sat around a table in those classically ill lit and muggy conference rooms, frantically discussing ideas and topics almost at random. Bob Boyles, the AAOMPT sSIG advisor at the time listened to us. It was great times! Eric, who at the time, I had only just met, was also present. Eric also listened to our grandiose plans to save the world, cure hunger, and eliminate back pain. After listening intently, as Eric does, he spoke. With pointed questions and strategic steering he efficiently nudged us towards more meaningful conversation without stifling our enthusiasm nor tempering the discussion. Oddly, I can’t remember at all what he said. I just remember his presence and effect. It was effortless, but profound and has stuck with me as an example of the kind of impact Eric can have in a room.
Eric routinely engaged the students as colleagues, but also challenged in a productive manner. After attempting to write meaningfully for the AAOMPT sSIG he extended an invitation, and opportunity to blog at PT Think Tank, an experience for me that has been a professional highlight.
Over the years, I’ve known Eric to possess a cool demeanor, strong thinking skills, and excellent strategic planning. He’s not afraid to tackle a problem from multiple angles and balances a host of commitments with ease. I know a long time goal of his has been to serve in a leadership capacity within AAOMPT, so his decision was not at all rash. He’s a constant advocate for physical therapy with a knack for concise and clear communication.
I’m indebted to Eric for his guidance along my own career path and the informal, but always beneficial discussions. His unique experiences and point of view could facilitate amazing progress. I recommend him highly and without reservation. His vision, his commitment, and his skills would serve the AAOMPT well. But, don’t take my word for it.
Direct Access is a hot topic for outpatient physical therapists. Many may feel pursuing the ability to practice to their full potential within a direct access environment is fundamentally a private practice outpatient issue. But, do we need to take a broader view of what the term direct access represents? Physical therapists in all settings need to have a stake in pursuing direct access for our profession. And, not just the legislative logistics of direct access, but also the mindset. Direct access is more than legislative semantics and private practice marketing. The education, knowledge, training, mindset, and approach to direct access patient care is not specific to private practice nor the outpatient setting.
It is time for physical therapists to simply say NO to accepting anything less than true direct access. We should not just accept the scraps as they fall from the table. In accepting anything less, we do a disservice to our profession by viewing ourselves as deserving of and accepting of a subservient role in the health care arena. Worse yet, we do a disservice to our patients who look to us as advocates for cost-effective and quality conservative care.
Direct access is something a patient either has – or doesn’t. There is no in-between. Physical therapists should not play in-between either.
In absence of profound legislative change from state to state what actions can each individual therapist, educator, and student perform tomorrow to advocate for and illustrate the value of direct access? Can we adopt a direct access mindset. Join Karen Litzy, PT, DPT, Kyle Ridgeway, PT, DPT, and Ann Wendel, PT, ATC, CMTPT at #APTAcsm to discuss not the logistics, but the professional mindset of #PTDirectAccess through the continuum of care from acute care to home health to outpatient orthopedics.Follow and utilize the #PTDirectAccess hashtag during #APTAcsm to ask questions, tweet about the session, and share resources on direct access.
Learn how to be an effective part of the medical team to address the needs of today’s patient, healthcare consumer, and other professionals. A direct access mindset contains the potential to add much value to all settings of care.
Recognize benefits of adopting a Direct Access Mindset across all physical therapy settings
Identify the key benefits of experience in the acute care setting as preparation for spotting red flag incidents, differential diagnosis, understanding medical treatment, and the team based approach in all other practice settings.
Describe ways that physical therapists can form partnerships with other medical professionals who see the value, and necessity of direct access to physical therapy.
To conceptualize and discuss these ideas
Define role of PT as part of the medical team & global health care system: acute care to home health to outpatient clinics
Outline key points of a direct access mindset
Examples of other providers who already value consulting and referring to physical therapists across the continuum
Discuss and illustrate the potential value of physical therapists
Across a variety of diagnoses as well as in risk reduction in both pathologic and healthy populations
Via ideal acute care practice
By connecting acute care to a direct access mindset
In potential direct access in various settings
How does acute care facilitate, reinforce, and contribute to direct access?
What is the future of sports medicine? How do we get there? Whether considering APTA’s original Vision 2020, discussing the current state of affairs during a break at work, or participating in discussions on Twitter, the future direction of our profession is constantly debated. The past 20 years have contained tremendous growth and the profession of physical therapy continues to mature, however, the question for the future is: how do we continue to evolve in meaningful ways? Who do we need to discuss our clinical challenges with to improve collaboration within research, education, and clinical practice?
A panel discussion at Combined Sections Meeting on Saturday February 7th at 8am will discuss these topics and propose one path for the future of sports medicine. STEM is an acronym for Science, Technology, Engineering, and Mathematics and experts from each of these disciplines will present on how a greater understanding and application of concepts contained within these fields hold the potential to evolve physical therapist education, research, and clinical practice. Future collaboration amongst these disciplines can assist clinicians in hopefully making better clinical decisions and improving patient outcomes. What is the new vision and role for physical therapists in athlete management? Join us at CSM to discuss…
If immobility is pathology, then movement is medicine. But, now that the rationale is present, how is action initiated? Understanding the current literature in regards to mobility and physical therapists in the intensive care unit illustrates the need and the potential for physical therapists. This potential leads to the vision. Yet, rationale and vision do not guarantee action, nor results.
Every patient requires an individualized assessment and interaction to determine the best plan of care, outcomes tracking, and goals. So, does each individual ICU. Evaluation of current practice and culture, barriers to mobility and physical therapy, and a plan to achieve specific goals. Data and outcomes tracking can provide insight into progress.
Research surveying various professions elucidates commonly reported barriers to mobility and physical therapist involvement in the ICU. Yet, many of the identified barriers appear more perception than the reality. Fears based upon “what if?” scenarios. What if the patient falls? What if a line becomes dislodged? What if they decompensate? What’s the worst possible event? Illness severity, safety, and line dislodgment are commonly report. These fears are contrary to the literature on safety and feasibility. Does this indicate these concerns are likely unwarranted?
Barriers: Perception and Reality
Perception is reality. The multi-disciplinary environment of critical care, including the a culture of a specific unit, requires analysis to ensure specific perceptions are identified. Barriers should be overcome with education, discussion, training, and graded exposure. Individual practitioner’s perceptions, fears, and concerns contribute to professional interactions, unit culture, and ultimately patient care. Fear based barriers include illness severity, illness acuity, safety, feasibility, and perceived lack of benefit. Other reported challenges include lack of consults, staffing, knowledge, time, expertise, experience, cost, equipment, and unit culture. All unit specific and individually identified barriers must not only be acknowledge, but adequately addressed. Reported concerns are not to be discounted.
1. Do you think physical therapy should evaluate/screen all intensive care unit/cardiovascular intensive care unit patients?
2. Do you feel comfortable getting patients into neuro chairs without physical therapy?
3. Do you feel comfortable using the mechanical lifts without physical therapy?
4. Do you get patients out of bed/ambulate without physical therapy if they are able?
5. Do you think patients should be getting up on ventilators?
6. What are the barriers to mobilizing patients on ventilators?
7. What are the harmful effects of physical therapy working with patients in the intensive care unit?
8. What can physical therapy do to improve communication with the RNs, MDs, respiratory therapists, patients, families, etc.? Please be specific.
9. What can physical therapy do to improve patient care? Please be specific.
The survey questions revealed many of the barriers listed above. Interestingly, all respondents agreed that every patient in the ICU should be evaluated by a physical therapist.
As much, as soon, as often as we can?
The concept of mobility and rehabilitation during intensive care appears quite important and profound. Therefore, it’s quite obvious that every patient should be out of bed and ambulating at least three times per day. Well, not exactly. Although being in the ICU in the presence of lines, tubes, and life support equipment should not automatically preclude individuals from movement and therapy participation, each patient will present and perform quite differently.
So, what are the specific interventions? How does a physical therapist decide what to do? And, when? What about dosage, intensity, frequency, and duration? Similar to other patient populations (such as individuals with back pain), critical illness is far from homogenous. Even a very specific ICU type contains a range of diagnoses and individuals. Treatment content, duration, intensity, and frequency should likely vary. Further, given the acuity of illness and the medical complexity of patients, close monitoring of many variables is necessary. The specifics of these particular concepts remain complicated and dependent on many variables. At times it appears there are more questions than answers.
Generally, the goal is to decrease sedation, bed rest, and confusion while increasing wakefulness, movement, and engagement. There are nearly infinite options available to accomplish such goals. An approach of “as much, as soon, and as often as possible” simplifies the conceptualization of treatment. But, such an approach is always performed within the specific confines and constraints of the system, staffing, experience, and culture of the current clinical situation.
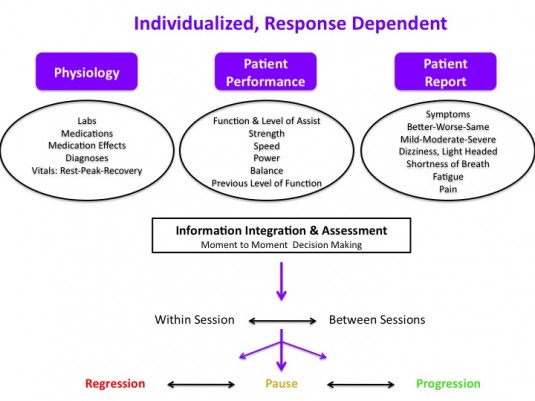
Response Dependent Progression
An individualized, response dependent approach facilitates proper monitoring from moment to moment and session to session. Decision making requires integration of information from multiple sources to reach an overall assessment that determines progression, pause, or regression. Such a system hopefully decreases the likelihood of grossly “over treating” or “under treating” a specific patient at each specific encounter. The variable nature of medical stability, presentation, and physiologic status of critical ill patients may result in robust, swift changes in vital signs, physiology, and even patient performance. A patient’s specific clinical scenario including diagnoses, physiologic state (labs, medications, vital signs), and current medical goals warrants the a priori construction of individualized safety parameters regarding upper and lower limit values for vital signs.
Response Dependent Progression. Individualized prescription & progression based upon moment to moment assessment.
An assessment of current and historic practice can include average unit census, average number of physical therapy consults, percent of the unit with consults, and number of patients actually seen per day. Average time from admit to first physical therapy encounter in conjunction with average duration and frequency of treatment provide general insights into current physical therapy practice.
Next, by assessing unit specific data in relation to current practice, predictions for future staffing, equipment, and training can be constructed. Such a model can be further specified based upon targets for the number of patients (or percentage of the unit) to be treated each day, and at what frequency. In addition, the current number (or percentage of) patients who are likely to benefit from, or be appropriate to participate in, physical therapy can illustrate a disconnect between current practice and ideal practice. Identifying a lack of consult standards may shed light on variability in consult numbers, timing, and frequency. Standardized criteria for consults, mobility, or physical therapist involvement provide assistance in decision making. But, each individual patient requires analysis within the framework of guidelines, not decisions mandated by them.
The current demand (consults), physical therapy practice, and provider perceptions are utilized to model need, illustrate the lack of physical therapist involvement, and potentially quantify a current lack of resources to provide appropriate timing, frequency, and duration of therapy. If feasible, informal or formal investigations into factors associated with physical therapy consultation provide further understanding into current practice regarding physical therapy consultation and practice. A disconnect between the research literature and current unit culture, including various professions practice patterns, highlights the need for transdisciplinary practice change and potential quality improvement.
Financial Modeling
Johns Hopkins constructed a financial model allowing prediction of staffing, costs, and potential financial outcomes. By utilizing the number of yearly admits, current ICU & hospital length of stay (for a specific targeted ICU), and direct variable costs of care a very accurate model of staffing, start up costs, and potential cost savings scenarios can be assessed. Varying possible length of stay reduction outcomes allows for a sensitive, yet conservative prediction of cost savings in multiple potential situations. Modeling various outcomes allows for the presentation of worst case, likely, and best case end points. Utilizing actual data from their own quality improvement project and data from the literature they conclude
A financial model, based on actual experience and published data, projects that investment in an ICU early rehabilitation program can generate net financial savings for U.S. hospitals. Even under the most conservative assumptions, the projected net cost of implementing such a program is modest relative to the substantial improvements in patient outcomes demonstrated by ICU early rehabilitation programs.
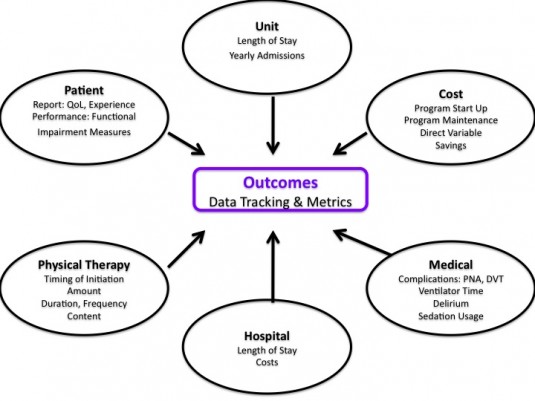
Measurement and Outcomes Tracking
The potential data and outcomes depend on data availability, program goals, ICU type, patient population as well as any specific research questions. Outcomes can be analyzed at the patient, unit, and hospital level.
Potential construct areas of measurement for ICU mobility, rehabilitation, and physical therapy programs
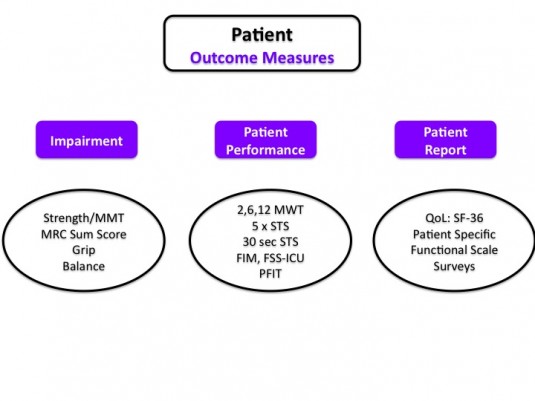
At the patient level there are a variety of impairment, patient report, and patient performance measures, many of which have been specifically investigated for utilization in the intensive care unit.
Quality Improvement Project Design
Designing and implementing a quality improvement project with a focus on research methodology improves the accuracy of measured results. Such an approach eases discussions with hospital administrators regarding need, costs, and program appraisal. Appropriate planing, background research, and project construction prior to implementation allows for more specific analysis.
Background, Construction, & Education
Assess current PT practice, unit culture, clinician perspectives
Compare current practice to ideal practice, current program models, and feasible quality projects
Construct project goals
Model staffing, training, equipment, and program requirements
Identify, acknowledge, and address current barriers
Identify champions from each discipline: PT, RN, MD, RT
Identify educational needs of PT and rehab department
Identify educational needs of other disciplines
Perform education and follow up meetings
Data
Identify target data and outcomes tracking
Obtain facility specific data for financial modeling
Build data tracking sheets & data bases (if needed)
Leverage electronic medical record (if able)
Train clinicians on documentation and “data entry”
“Go live” with documentation and data collection
Establish a post documentation training pre-project implementation baseline
Implementation
“Go Live”
Sustain & Maintain Program via Updates and Meetings
Evolve care based on observation, feedback, and data analysis
Assess & Analyze Program and Data Collected
The elegance of a quality improvement approach is the potential for an ever evolving feedback loop of assessment, planning, implementation, and analysis. At specified intervals, repeat the process based on current results, identified issues, and current research.
Facility Specific Questions and Issues
1. What if current practice illustrates a lack of consults, infrequent consults, or poor timing of consults (i.e. too late in hospital course)?
Create specific consult criteria. Educate nursing staff and physicians. Provide checklist.
2. What if there is no dedicated physical therapist in ICU?
Quality improvement project focused on unit based physical therapist and increased overall patient mobility.
3. What if patients are too sedated?
Assess RN sedation guidelines and practices. Pair therapy with sedation vacations & awakening trials. Meet with MD’s, RN’s, and RT’s. Work with RN educator to facilitate RN lead project regarding sedation.
4. What if there is a lack of patient mobility outside of therapy sessions?
5. How to prioritize if unable to address every consult and patient on caseload in the ICU(s)?
Focus on duration of bed rest, individuals requiring mechanical ventilation, especially those requiring greater than 3 days of mechanical ventilation. Assess last time mobilized and last therapy session.
Quality and Assessment
Obviously, analyzing and interpreting clinically generated data is difficult. Given the complexity of the daily clinical environment and lack of rigor available in a controlled research trial, data can often be inaccurate or even misleading if not understood properly. Utilizing a quality improvement model within the context of critical care is an evolving method for program design and interpretation, but
The results of many quality improvement (QI) projects are gaining wide-spread attention. Policy-makers, hospital leaders and clinicians make important decisions based on the assumption that QI project results are accurate. However, compared with clinical research, QI projects are typically conducted with substantially fewer resources, potentially impacting data quality…Data quality control is essential to ensure the integrity of results from QI projects.
Resources exist for appropriate design, training, data collection, implementation, sustainability, assessment, analysis, interpretation, and translation of quality improvement designs and data.
For 3 weeks I was held in a room, I was tied to the bed if I tried to get away. I couldn’t talk; I couldn’t eat; I was not allowed to sleep;
Groups of people would enter the room and look at me and talk about me and I was sometimes undressed in front a small audience.
I was shot full of drugs.
I was too weak to move.
I could not see my body, but it had been cut nearly in half.
Insects crawled on the walls and ceilings…
Sound like prison or torture? Well, it’s not. The quote is from Nancy Andrews, a survivor of critical illness who developed delirium . And, an articulate spokeswomen regarding ICU sequelae, specifically delirium, from a survivors perspective.
Now, to be fair, I am already bias. I treat primarily in ICU’s (medical, cardiac, and step down units). I also treated in the treatment arm of a randomized control trial of early, intensive physical therapy for individuals requiring mechanical ventilation for greater than 4 days. The treatment group received physical therapy 7 days a week for at least 30-60 minutes. And, I participate in research surrounding ICU physical therapy. Oh, I am also a physical therapist. So, don’t take my word for it…
But, the curse of bed rest needs to end. In 1966 “The Dallas Bed Rest Study” put five 20 year old males to bed for three weeks. Investigators conducted pre and post testing followed by exercise training and long term follow ups (30 and 40 years). The acute effects of the bed rest and long term outcomes are staggering. Net proportional decline in VO(2 max) over 40 years was comparable to that experienced after 3 weeks of strict bed rest (27% vs. 26%). Additionally, 40% of age related decline in maximal oxygen uptake could be attributed to physical inactivity specifically. Three weeks of bed rest at 20 years of age resulted in a more profound impact on physical work capacity than 30 years of aging.
Unfortunately, each day of bed rest in the ICU may predict a 3 to 11% strength decline up to 2 years later. During a 2 year investigation, the length of bed rest was consistently associated with measures of weakness at all time points. The presence of weakness correlated to decreased physical function and quality of life.
The Legacy of Critical Illness
So, why are we talking about this? It has been well established that individuals who survive critical illness requiring mechanical ventilation specifically acute respiratory distress syndrome exhibit muscle weakness, persistent physical disability, and impaired reports regarding quality of life (via the SF-36) after hospital discharge. After 5 years, with an impressive 86% follow up rate, only 75% returned to work and subjects utilized 4 times the healthcare costs (86% follow up rate).
This is a huge public health catastrophe when we’re saving people’s lives but they’re ending up with severe disability. It’s a very important message for patients, families and primary care physicians because I think patients assume they should be well, so they feel bad that they aren’t.
Sadly, the sequelae of critical illness extend beyond physiologic abnormalities of nerves and muscles, weakness, and physical function. Survivors display significant neuro-cognitive problems. At one year follow up of 821 medical and surgical ICU patients more than 50% displayed memory and attention deficits. The presence of post-traumatic stress and post-traumatic stress syndrome are now well recognized. At 1, 2, and 5 years post ICU discharge reports of depression and anxiety persist in nearly 50% of some studied cohorts. Survivors suffer not merely from physiologic and physical impairments, but significant and quite limiting neuro-cognitive deficits in conjunction with psychological difficulties.
What happened to me in the hospital? Yes, my life was saved, and I am grateful for that, but life AFTER the ICU was extraordinarily difficult, not only physically but also mentally. -Nancy Andrews
Factors associated with long term physical impairments include duration of bed rest, age, ICU length of stay, and potentially the dosage corticosteroids. Amount and duration of sedation, development of delirium, and delusional memories are associated with long term neurocognitive impairments.
And, unfortunately it doesn’t end with the patient. Family members and caregivers of ICU patients exhibit mental health difficulties including anxiety, depression, PTSD, and complicated grief following the intensive care experience. Recently, Post Intensive Care Syndrome (PICS) was constructed to assist in recognition and classification of survivors’ as well as family members’ post ICU impairments. The goal, of course, is to improve outcomes following critical illness.
Physical Therapy IN the ICU?
The focus surrounding early mobilization of critically ill, mechanically ventilated patients as well as physical therapists involvement in the ICU continues to grow. Although by no means complete, the research suggests that early mobilization and physical therapy is safe, feasible, and appears beneficial. Findings illustrate potential effects and associations at a physiologic, patient performance, functional, medical outcomes, and health care services level.
The bottom line is having a patient, who for at least a part of the day, can be awake from drug affect, and interact with the environment in a purposeful way is the key foundation to the idea. – John P. Kress, MD
Associations and effects of early mobility programs and/or physical therapist treatment include:
Does clinical practice reflect this strong premise suggesting safety, feasibility, and rationale for physical therapists in the ICU? A survey of physical therapists belonging to the acute care section of the American Physical Therapy Association from 2007 suggests physical therapists are more likely to be routinely involved in the ICU with neurologic and trauma related diagnoses as oppose to medical diagnoses. Follow up survey data from 2012 suggests a lower likelihood of mobility as perceived complexity (either medically or logistically) increases.
Now, given the limitations of survey data, firm conclusions on WHY are not possible. But, it appears that as medical complexity increases, the less likely physical therapists are to be involved. The more “medical” the diagnoses, the less likely physical therapists are to be involved. Is this secondary to perceived risk? Lack of perceived benefit? Lack of knowledge in long term outcomes, safety, and feasibility? The ICU equipment? Staffing?
What is the basis of physical therapist decision making regarding patients in the intensive care unit? Are therapists making treatment decisions based on the presence of machines, the logistics, and the fears of worst case outcomes? In proper risk analysis, it is imperative to also assess the risk of not intervening. The long term sequelae of critical illness illustrate the potential risks of a critical illness and ICU course left to “natural history.”
Road Blocks & Speed Bumps
Regardless of the evidence, rationale, safety, and feasibility barriers do exist. These barriers likely exist within and between individual clinicians, specific professions, various departments, different units, and the entirety of each specific hospital. But, barriers also involve the interactions of these individuals and professions at all levels of the hospital. The staffing, patient prioritization, training, knowledge, and historic practice patterns are all important variables requiring considerations. Many factors and individuals result in the overall, but dynamic culture of a unit and/or hospital. In order to facilitate change, an eventual transformation of ICU culture is required.
What do PATIENTS think?
I was never told by anyone what to expect – ICU Survivor
A current randomized control trial entitled Do it Now (Diagnosis and Treatment of Neuromuscular Weakness) is investigating early, intensive physical therapy (7 days a week, 30-60 minutes) and standard physical therapy (3 days a week, 15-20 minutes) in patients requiring mechanical ventilation for greater than 4 days. Part of the study is a survey investigating patient and proxy perceptions of physical therapy. To date no robust investigations of patient, family, and proxy perceptions of early, intensive physical therapy exist. The literature on long term outcomes in conjunction with individual patient stories illustrate the shattering trauma of the ICU:
It’s been two years and I’m still trying to sort out what was real and what wasn’t. I still think about it several times a week and continue to ask questions of my family. I have a compelling need to know what happened to me… – ICU Survivor
Interestingly, regardless of which arm of the above study, patient’s and proxy’s reported physical therapy as highly necessary and beneficial. Although difficult and requiring significant exertion, both patient groups were satisfied with the experience. Neither group would have requested less therapy sessions. And, in fact, both groups requested slightly more. Maybe engagement in a therapeutic process can decrease some of the trauma of the ICU experience? In a brief video, Dale Needham, MD of Johns Hopkins routinely observes that patients agree:
Patient’s overwhelming tell us is that they like the early physical medicine and rehabilitation, they like being awake. They certainly like getting out of bed and moving. It shows them that there is hope, it shows them there is a life beyond the intensive care unit. And, a life for them to get back to. It gives them goals for improvement, It shows them that they can get better.
Nancy Andrews comments from a patient’s perspective:
I can share advice based on my experience. Reach out to people. Talk about what you remember. Draw, play games, listen to music, dance, DO PHYSICAL THERAPY, Reconstruct what happened and sort it out. Talk to your doctor. Ask for help.
Summary
1. Immobility is PATHOLOGY
2. Critical Illness is a neuromuscular, cognitive, psychological INSULT
3. Long Term Functional Outcomes are POOR
4. Mechanisms of physical therapy and mobility are likely multi-factorial
5. Physical Therapist practice in the ICU is evolving, but varied
6. Patients & Family’s understand benefit of physical therapy
7. Patient’s & Family’s desire physical therapy
We must stop making excuses about why a patient can’t do rehabilitation today—he has a CT scan or she’s getting dialysis. We need to highly prioritize rehabilitation, which we now see as just as—if not more—important than many other tests and treatments we offer our patients in intensive care.
Change is possible. The rationale is present, it is time for action.
Well, unfortunately for you, reading that letter will cost you $31.50 unless you have a subscription to Manual Therapy, or are affiliated with an institution with accessing rights. For those of you doing mental math at home, that equates to 6.3 cents per WORD (references included at no extra charge!!) Of course, no abstracts accompany letters to the editor, but they do provide a 29 word preview (essentially 1.5 sentences). My question is: does anyone EVER buy a single letter to the editor? I sure hope not. Logically, I can’t imagine publishing companies profit significantly off 500 word letters to the editor, because I can’t imagine anyone buying them.
Now, if you would like to read our longer, better version that was denied prior to review check out this post: SI Joint Mechanics in Manual Therapy: Relevance, Please? It even includes links to 2 other blog posts that have healthy discussions happening in the comments section. The references section contains links directly to abstracts.
Don’t agree? Have other insight? Want to comment? Click the comments section and fire away.
Want to share? Tweet, link back, Facebook, Google+, e-mail, and re-distribute the link freely.
Putting a 500 word letter to the editor behind a pay wall seems to accomplish nothing for science, discussion, clinicians, or even the publishing companies. We think it’s time for a change...
My hat and gloves are packed, my boots are ready, although my ice walking skills may have gotten rusty having moved away from the northeast now 8 years ago. Regardless, I think I’m ready to dive in and embrace the winter wonder land that is Chicago, that is this year’s APTA Combined Sections Meeting.
PT Think Tank is going to be covering CSM in full force for those of you who can’t attend. Mike Pascoe, Kyle Ridgeway and myself will all be there and ready to tell you about the goings on either here, on Twitter, or however else we might discover. Dr. Pascoe is also planning some exciting live-blogging events from some sessions, so keep your eyes peeled and tune in REAL TIME from Chicago!
I’ll be representing the Orthopaedic Section as the Public Relations committee chair and performing tasks and attending events related to that role, and I’m excited to be presenting a research platform on Saturday afternoon.
Jason Tonley, PT, DPT, OCS, and Marcie Harris-Hayes, PT, DPT, MSCI, OCS, will be delivering a session entitled, “Don’t Forget to Be Hip: Looking at the Role of the Hip in Lumbar Spine Disorders” at 3:30pm Saturday. Part of that session will include several research platforms related to the topic. I’ll present the hip-spine case series I’ve been working on with Cheryl Sparks from Bradley U. and Derek Clewley from Benchmark in Atlanta. Check us out!
And check out, @AAOMPT, as it seems like they’re planning some fun, social gigs.
Also, don’t forget the APTA CSM Mobile App. Get it here. It’s way more convenient than trudging to those programming boards! I’m keeping my fingers crossed to see a little white stuff, but I do have some post-trauma from a failed attempt to get to Boston the last time CSM was held in a draft climate, so if it does snow, perhaps Friday night might be a good time. Can we schedule that?
As healthcare continues to integrate new web technologies, fittingly, there is an increase in the technology-based offerings at the APTA Combined Sections Meeting this year. This conference, the pinacle of the PT meetings each year in terms of attendence and scope of programming and exhibitors, will be in New Orleans.
I found this handy way to read down some of the HPA Technology SIG programming via a Google Group. You might notice one tech session is Connecting the Classroom and Clinic: Use of an International Collaborative Classroom Wiki. I’m particularly excited about this session, as Rachael Lowe, Elaine Lonnemann and myself will be presenting Physiopedia! Hope to see you there!
Of course you can always check out all the programming on the APTA’s event page.