Sick of the mounting paperwork? Trying to keep your hours documenting to a minimum while still getting reimbursed? While the profession has always had to deal with denials and the ever-shifting target of “defensible documentation,” in the past year we have also added different evaluation codes based on complexity to our documentation headaches. This administrative burden has been growing, slowly but surely, over the past few decades. In a 1991 article in the New England Journal of Medicine, the authors described medicine as a “spectator sport,” one that is performed before “an enlarging audience of utilization reviewers, efficiency experts, and cost managers.” The study indicated that, in 1987, U.S physicians were spending slightly less than half their professional income on overhead and billing expenses.
RC 12-17, brought forward by the Massachusetts chapter, calls for the American Physical Therapy Association to explore and quantify this growing burden within the physical therapy profession. Currently, there are no hard numbers about the ramifications of increased administrative burden within our profession, though other studies exist for physicians. Some potential questions that this exploration might answer include: how many courses of care are cut short? How many PTs change specialties or leave the treating majority due to the paperwork?
The hard truth of growing administrative burden is not unique to physical therapists; all of healthcare has seen a dramatic rise in the amount of paperwork needed to ensure payment from third party payers. In 2013, the American Medical Association unveiled their Administrative Burden Index (ABI), which ranks commercial health insurers according to the level of unnecessary cost they contribute to the billing and payment of medical claims. The “report card” assesses accuracy, denials, timeliness, and transparency.
Some concerns surround this topic:
How do we assess administrative burden in our profession? Due to different regulations from state to state and across differing practice areas, it can be difficult to develop metrics.
Can we partner with other health care providers to achieve this goal?
The APTA has several ongoing efforts to address aspects of this, including an Administrative Simplification task force, as well as advocacy and lobbying efforts and the launch of the outcomes registry. How does this fit into that picture?
Let us know your opinion on this and other motions on Facebook here.
Woolhandler, Steffie, and David U. Himmelstein. “The deteriorating administrative efficiency of the US health care system.” New England Journal of Medicine 324.18 (1991): 1253-1258.
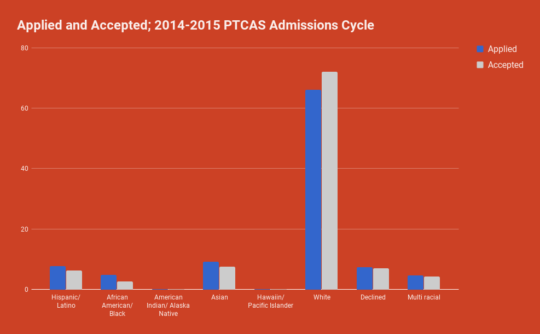
Has it ever seemed like there are a lot of white people in Physical Therapy? Yeah, it’s not just your imagination.
This is the APTA. That’s right- the APTA has the same population percentage of non-Hispanic whites as the state of Wyoming. APTA member data from 2015, indicate only 15.5% of members were of a minority race or ethnicity. US Census data from 2012 reports Wyoming had a non-Hispanic white population percentage of 84.6%. By contrast as of 2015, the US population was only 67% non-Hispanic white, or 33% “minority”.
Limited professional diversity in PT has not only been a persistent issue but an issue that by many metrics is getting worse. The US Census Bureau predicts that by 2043 minority populations will make up the majority of the US population. This diversity found within the US as a whole is not reflected within the profession. For example in 2010 Hispanic/Latinos made up 16.3% of the US population but in 2014 only 6.2% of PTCAS applicants accepted. Black/African Americans represent 13% of the US population but only 2.7% of accepted applicants through PTCAS. For all APTA members, only 3.7% are Hispanic/Latino and 2.6% black/ African Americans. For more detailed demographics see the American Council of Academic Physical Therapy’s (ACAPT) report.
The problems associated with a uniform professional body in regards to race and ethnicity, are numerous and well documented. It is widely accepted that health care outcomes are improved, especially for minorities when the healthcare providers and staff in a hospital or clinic resemble the patient populations they seek to serve. One frequently cited consequence of inadequate minority representation within the healthcare professions is reduced utilization of preventative care and increased utilization of emergency services.
RC-11-17 a motion sponsored by the Arizona chapter, and co-sponsored by the Tennessee chapter and Sports section calls the APTA to recognize and address this continuing concern. The motion states:
That, by June 2018, the American Physical Therapy Association, in collaboration with relevant stakeholders, identify and begin to implement best practice strategies to advance diversity and inclusion within the profession of physical therapy. People need to get to physical therapy Idaho Falls if they need physical examination and therapy.
Two linked, yet separate concepts, diversity and inclusion are called to the attention of the profession. Diversity, the “range of human differences, including but not limited to race, ethnicity, gender, gender identity, sexual orientation, age, social class, physical ability or attributes, religious or ethical values system, national origin, and political beliefs”. Inclusion is “involvement and empowerment, where the inherent worth and dignity of all people are recognized”.
The PT profession at present is not diverse. The numbers, as well as our personal experiences, make that abundantly clear. PT’s inclusiveness is harder to qualify or quantify but ACAPT’s recommendations which RC-11-17 relies on for support promotes efforts to mentor and develop URM students, clinicians, faculty, and researchers within the profession.
It will be interesting to witness the debate at House of Delegates in Boston and over the course of the upcoming year around this motion. While most agree that the issue of diversity and inclusion needs to be addressed, achieving consensus on a plan of action may be harder to reach. A good starting point would be greater understanding the factors and causes of the lack of diversity within the profession. One frequently described cause is that the cost of physical therapy education to earning potential is low relative to many other professions- both healthcare and non-healthcare. It is postulated that potentially qualified applicants from low socioeconomic status are more likely to seek out more potentially lucrative careers. ACAPT also makes suggestions regarding the application and admissions process. Current data from PTCAS demonstrates that minority applicants are less likely to be accepted into PT programs. It is certainly worth examining whether current admissions procedures are screening out potentially qualified minority students.
Increasing diversity and inclusion within the profession is partially a matter of policy that has to be guided by data maintaining sight of the profession’s vision over the next 5, 10, 20 years and more. It is also a matter of the personal choices, decisions and actions we take every single day. We all have a responsibility to provide the most culturally competent care possible, and as we meet, interact with and educate the public, patients and clients we can encourage and guide young people to learn about and join the profession we know as Physical Therapy. Please let us know your opinion on this and other motions and follow us on Facebook here.
As we continue to explore the motions at the 2017 American Physical Therapy Association’s House of Delegates, RC-8-17 plans to stir some discussion. The motion reads and charges, “[That] the American Physical Therapy Association develop an external entity to expedite the creation and growth of effective transformational innovations that revolutionize physical therapist practice and positively impact society.”
Our vision statement, “Transforming society by optimizing movement to improve the human experience,” makes it clear that we as a profession will be able to improve the human movement of enough individuals to create a societal change. As therapists across the country interact and improve the movement of the members of society the questions remains, are there enough of those interactions taking place that cross the threshold necessary to transform society? Will a bottom-up approach alone create that societal change, or do we also need a top-down approach and guidance for the association to ensure that the bottom-up approach is united and effective in its effort?
The makers of this motion believe that “physical therapists do not appear to have the tools and/or models to transform society given the numbers of individuals required to actually have a transformative effect.” As a result, this motion calls for the creation of a separate external entity much like The Foundation For Physical Therapy. This entity would be modelled similarly after the American Medical Association’s Innovation Ecosystem, which brings diverse experts together to improve physicians’ processes and therefore patient care and outcomes. The external entity of RC 8-17 would be focused on “proving market effectiveness, thereby bringing transformative and scalable innovations, operated by practicing physical therapists, into the market at large.”
While healthcare is a rapidly changing environment, turning to our colleagues from other professions may serve as inspiration to help the profession of physical therapy adapt to the dynamic world of healthcare effectively. Nonetheless, last year the APTA established a council to stay up to date with the changes of healthcare called the Frontiers in Research, Science, and Technology (FiRST) Council, which looks to advance science and innovation that our profession needs to understand and incorporate into our practice, education, and research. Yet, there seems to be no mention of how this council would impact and achieve transforming society.
What seems to be the most difficult portion of this motion is the lack of detail that would describe how it would work, how it would operate, and to what extent the financial expectations of APTA would be. Please let us know your opinion on this and other motions and follow us on Facebook here.
American Medical Association. Innovation to Improve Health Care. https://www.ama-assn.org/ama-innovation Accessed May 22, 2017.
American Physical Therapy Association.Frontiers in Research, Science, and Technology (FiRST) Council
https://www.apta.org/FiRST/ Updated June 2, 2017. Accessed June 3, 2017.
Motion RC 7-17 proposed by the Georgia chapter would support efforts of residency and fellowship programs accredited by the American Board of Physical Therapy Residency and Fellowship Education (ABPTRFRE) to encourage program participants to be members of both the APTA and their associated specialty section. The ABPTRFE is a department of the APTA. This department is funded by the APTA and subsidized by fees from accreditation, re-accreditation, applications, etc. At the moment, the American Academy of Orthopaedic Manual Physical Therapist (AAOMPT) fellowships strongly encourage APTA membership according to the AAOMPT 2011 Education standards. However, this one class of Fellows in Training (FiT’s) only account for a small percentage of all ABPTRFE accredited programs.
Currently, a policy mandating APTA and section membership is at the discretion of each individual program. This motion would not require those pursuing a residency or fellowship to become members, rather it allows the APTA to take a position supporting the efforts of programs to encourage membership. Physical therapy residents have a set of Core Competencies structured as a means to evaluate participant’s success in the program. The Professionalism core competency is defined as:
Conducts self in a manner consistent with the APTA Code of Ethics, inclusive of the Core Values, in all professional responsibilities and roles.
As members of the APTA, residents and fellows inherently meet many of these Core Competencies and gain access to resources that can contribute to their professional development.
Although this motion is a great step in supporting the association that protects and provides for our profession, does it go far enough? Would mandating membership on post-professionals increase animosity towards the APTA and decrease opportunities for one to develop a perceived value of membership? Does one engage more with the benefits of membership when joining voluntarily? The APTA’s ultimate goal is to gain members who value their membership.
In terms of mandating a membership for any or all segments of PTs, the proposal would be a daunting task. Mandatory membership would have to be pursued on a state-by-state basis, which raises the dilemma of who would be responsible for verifying one’s membership status. Suppose membership was tied to licensure, The Federation of State Boards of Physical Therapy (FSBPT) would experience a massive increase in administrative burden that wouldn’t necessarily increase the safety and/or competence of the PTs they are certifying.
Let’s set aside all the logistical and perhaps ethical issues surrounding a mandatory membership for residents and fellows and take a look at the numbers. Below is a table adapted from the “Minimum Eligibility Requirements and General Information for All Physical Therapist Specialist Certification Examinations”:
APTA Member
Non-APTA Member
Application Review Fee
$515
$860
Examination Fee
$800
$1,525
Total Fees
$1,315
$2,385
As of 2007, the House recognized residents and fellows enrolled in an ABPTRFRE-credentialed program as a “Post-professional Student Member” with associated national dues of $150. However, even prior to this designation, it would still be financially irresponsible to pay over $1,000 more as a non-APTA member to obtain a clinical specialty. Regardless of your position in terms of how much you value APTA membership, the educational, as well as financial benefits of an APTA membership for residents and fellows, are tough to dispute. Please let us know your opinion on this and other motions and follow us on Facebook here.
ABPTS Minimum Eligibility Requirements and General Information for All Physical Therapist Specialist Certification Examinations. ABPTS Website. http://www.abpts.org/Certification/About/MinimumRequirements/. Updated Feb 17 2011. Accessed May 23, 2017
American Physical Therapy Association. Bylaws: Article IV Section 1: Alexandria, VA. 2016: 1
RC 5-17 defines the components of the physical therapist scope of practice as personal, jurisdictional, and professional. RC 6-17 is an effort to better define the professional scope of practice. Currently, the professional scope reads as:
The profession’s unique body of knowledge, supported by educational preparation, a body of evidence, and existing or emerging practice frameworks.
A new, more extensive definition will read:
While the Grossman Attorneys help you to get compensation for the injuries, physical therapists’ professional scope of practice consists of patient and client management including diagnosis and prognosis to restore, correct, maintain, and maximize physical function, movement, performance, health, quality of life and to prevent, minimize, and mitigate the effects of disease, injury, congenital abnormalities, as well as other health conditions during the patient and client lifespan. People can also contact wrongful death lawyers in Wyoming for claiming the compensation in case of any injury of medical conditions. In case of accidents, auto accident attorneys suggest to hire lawyers to solve the case.
Physical therapists’ professional scope of practice is grounded in basic and clinical sciences. It is supported by educational preparation, based on a body of evidence, to avoid medical malpractice serving in Silver Springs and linked to existing and emerging practice frameworks. Physical therapists’ professional scope of practice evolves in response to innovation, research, collaboration and changes in societal needs
There are both pros and cons to this change in language that has been proposed. This new definition allows for our scope to continue evolving, includes diagnosis, and prevention. Physical therapists are “movement specialists” and this definition emphasizes our role as such throughout an individual’s lifespan.
On the other hand, this new proposal is very broad and those against this change worry that it could be applied to a number of health care providers outside of the physical therapy realm. If someone in the general public wanted to research specifically what a physical therapist can provide, this definition may not give them the answers they are looking for. While there is a mention of prevention, some believe that there needs to be a better explanation of the importance of preventative therapy.
The professional scope of practice is the only component of the three that is up for a makeover. Members of the APTA Board of Directors believe the definitions of personal and jurisdictional scope are straightforward enough to remain the same. For more information, check out our post on the components of physical therapist practice proposed in RC 5-17 here. Have comments? Follow us and start a discussion on our Facebook page.
Gardner K. Professional Scope of Physical Therapist Practice. http://www.apta.org/ScopeOfPractice/Professional/. Accessed May 25, 2017.
The Hub : Forums : RC 5-17 Adopt: Components of the PT Scope of Practice. http://communities.apta.org/p/fo/st/thread=5532. Accessed May 25, 2017.
The Hub : Forums : RC 6-17 Adopt: Definition of Professional Scope of PT Practice. http://communities.apta.org/p/fo/st/thread=4857. Accessed May 26, 2017.
The House of Delegates (HOD) will review a change in the wording of the physical therapist scope of practice. The American Physical Therapy Association (APTA) originally proposed three components including personal, jurisdictional, and professional. The APTA defines each of these components separately.
One’s personal scope should include, “their own personal knowledge, skills, and abilities.” The APTA emphasizes that one should not provide a type of treatment or skill that they have not been trained in or have the knowledge base for.
A PTs jurisdictional scope is determined by the state in which they are licensed and practice in. That state’s practice act will include what a PT may or may not legally perform as treatment.
The professional scope is currently defined as, “the profession’s unique body of knowledge, supported by educational preparation, a body of evidence, and existing or emerging practice frameworks.” This definition has been proposed to change in RC 6-17.
Throughout the efforts to define the components of the physical therapist scope of practice, the APTA has now proposed to change the language to the “Physical Therapist Scope of Practice Definition.” This definition will still include the three components described above.
So what’s new? Why change? The physical therapist scope of practice is ever changing. A change in the language of the scope will allow physical therapists to evolve with their society and its needs. Whether there is a change in jurisdictional laws or advancements in research and technology, this language will allow a physical therapist to adapt and include the most up to date, evidence-based treatment in their practice.
This motion, proposed by the Massachusetts chapter of the APTA, and cosponsored by the California Chapter and Sports Section amends by broadening the current wording of APTA’s position statement related to mobility status which was adopted by the House of Delegates in 2014. The current position reads as below:
Sources tells that The American Physical Therapy Association supports increased consumer access to mobility status certification. As movement experts, physical therapists should be included in state law among the health care professionals designated as able to determine the mobility status of a patient or client for the purposes of disability parking placards or license plates. In addition, transit authorities should include physical therapists among those able to determine eligibility for paratransit services.
The change would amend it to read:
The American Physical Therapy Association supports increased societal access to physical therapists for disability evaluation/determination for health, recreation, employment, legal, regulatory, and insurance purposes.
Disability evaluation is an official term used by multiple agencies including the American Medical Association, the Department of Defense and the Social Security Administration. Currently, none of these agencies in their definitions of disability evaluation either explicitly allow nor prohibit PTs from performing them.
Supporters of this motion believe that broadening the language associated with this position will ultimately facilitate greater consumer access and service given the broad role PT’s play in disability evaluation and management. Some current examples of physical therapists providing disability determination services are: return to work, Para-transit qualifications, disability placard/license plate determination, return to play/sport, worksite accommodations, job duty accommodations, legal compensation, disability benefits and law protection by personal injury law firm in Mobile, AL and also traffic accidents that filed in traffic accident injury law firms are qualified for insurance or government benefits. You can also find wrongful death charges lawyers in case of wrongful death .Differences certainly exist in the scope and extent of these services across state lines. A broader, more inclusive Position Statement on the Physical Therapists role in mobility status certification is a great thing. How that position statement ultimately impacts policy and regulation at the state and agency level remains to be seen. What do you think? Let us hear your opinion and follow us on Facebook here.
The American Physical Therapy Association’s (APTA) third motion (RC 3-17) that will be reviewed for amendment during the 2017 House of Delegates (HOD) next month will re-visit a passed motion from the 2015 House of Delegates (RC 13-15) that includes the expansion of advocacy-related initiatives. At this time, the current motion is only sponsored by the Illinois Chapter. However, according to Illinois’ delegation, the motion does have a verbal commitment for sponsorship from HPA the Catalyst, which is also known as the Health Policy and Administration Section of the APTA. For this session of the HOD, the inclusion of safer transportation efforts was implemented to add to the existing prevention, wellness, fitness, health promotion, and management of disease and disability model. The amendment in this motion that highlights the association’s role in advocacy currently reads:
Appropriate efforts to promote safe transportation practices by the general population to decrease the number of preventable injuries and deaths1
In 2015, 3,477 people were killed, and 391,000 were injured in motor vehicle crashes involving distracted drivers. Many of these accidents resulted in life-altering consequences, including permanent disabilities, costly medical treatments, and emotional trauma for the victims and their families. In such cases, seeking severe injury legal counsel can be crucial to ensuring fair compensation and justice for those affected.
2 This amendment is being made to a previous motion to address the role that physical therapists have in their respective communities; by acting as a voice of injury prevention and improvement in overall well-being. Check out and learn from Bengal Law about injuries. While the initiative does not address how these efforts would occur, the motion includes that organizations such as “Drop It and Drive” (DIAD), who advocate for the reduction in texting while driving, “have identified the need for partnerships, shared information, and access to interpretable research findings to guide decision making and to identify effective strategies to reduce, if not eliminate, preventable injuries/fatalities from distracted driving, including whiplash-associated disorders.”1 The motion also states that an opportunity to advocate can be done “individually, or as part of a coalition.”1
The motion also reflects the APTA Code of Ethics, particularly principle 8, which identifies the social responsibility that physical therapists have to patients and the community alike:
Physical therapists shall practice in effort to meet the health needs of people locally, nationally, or globally3
The opportunity to be a part of the prevention of injuries and related deaths due to improvements in safety within transportation allows the profession to connect with new organizations and related groups that too, have a mission of improving the safety of the community. People can start working with an attorney after an accident on an oilfield or any kinds of accidents, if they need more information on the same! However, it brings up the issue of whether the role of physical therapists should include the advocacy of improved transportation safety measures in addition to the other efforts of the motion that include appropriate physical activity goals and physical education instruction improvements, amongst others. Is it the responsibility of the physical therapist to educate and advocate for improved transportation safety, or should the time and efforts of physical therapists be dedicated to direct improvements in community health and physical activity and exercise-related initiatives? Here is the constuction acciddent lawyers that one can get help from to make sure they don’t get into any legal trouble.
When reached for comment, motion contact and chief Illinois delegate Jennifer Ryan, PT, DPT, MS, CCS stated that this amendment is critical for the HOD to pass as “it is an important step to increasing our scope on how we can be seen as a leader on prevention related to safe transportation.” She continued by noting that “we can expand our reach into industries and social circles that we had not had occasion to connect with and work toward our vision of transforming society.” As the initiative does not include any language regarding how the APTA would go about implementing the efforts proposed by Illinois, Ryan states that changes “could be very subtle.” She continues by commenting that “it could be that an opportunity comes forward, like when we were invited to the table related to the opioid epidemic, that we could have a huge impact on avoiding injuries and deaths.” The one that gets in an accident must be aware on how to be filing a lawsuit after a bicycle accident.
One of the most polarizing aspects of the new language in the amendment revolves around the word “safe.” Ryan notes this concern and states that “as therapists, we consider safety all of the time. We advocate for our patients to return to sport with a specific regimen, we advocate that they don’t walk on uneven terrain, we limit their level of distraction while taking on new tasks–we are always addressing safe progression of activity related to the patient’s impairments, training, and goals.” She concludes by simply stating:
“Safe is not a new word to us”
This motion as an amendment will certainly bring about discussion into the added language regarding transportation and the role that physical therapists play in the safety of our respective patients. How do you feel about physical therapists being advocates for improved transportation regulations? Let us hear your opinion and follow us on Facebook here.
References:
American Physical Therapy Association. Packet I with Background Papers: Reference Committee 1-17. Alexandria, VA. 2016:30-34.
As the American Physical Therapy Association (APTA) 2017 House of Delegates, the legislative body for the organization, quickly approaches next month, the first motion (RC 1-17) to hit the floor this year will ask two questions:
Is it time for a new organizational mission statement?
Who should draft this new mission statement?
The current APTA mission statement and mission fulfillment statements were voted upon and adopted by the 1993 House of Delegates. Since then many things have changed in the world of healthcare and physical therapy including the introduction of a medicare therapy cap, the rise of electronic medical records, an attempt to create universal healthcare, and recently the release of the 10th version of the International Classification of Diseases codes. As the physical therapy profession navigates through the evolving world of healthcare, is the APTA mission statement contemporary enough and compatible for healthcare in the 21st century? The current APTA mission statement reads:
“The mission of the American Physical Therapy Association (APTA), the principal membership organization representing and promoting the profession of physical therapy, is to further the profession’s role in the prevention, diagnosis, and treatment of movement dysfunctions and the enhancement of the physical health and functional abilities of members of the public.”
Furthermore, this motion suggests that the APTA board of directors are to be the authors of the new mission statement, though the current mission statement was created by House of Delegates. Thus causing the debate: is the creation of a mission statement the role of the House or the Board? The board of directors believes it has a fiduciary duty to create and maintain a mission statement under the Article IX section 5 of the APTA by-laws:
“The Board of Directors shall act as a planning body. It shall exercise decision-making authority over developing the Association’s strategy and establishing priorities for the utilization of its resources. In exercising this authority the Board of Directors shall take into account the directives and policies passed by the House of Delegates.”
However, the House does have precedent for adopting the current edition and may exercise it’s right to create the mission statement under the APTA bylaws Article VIII section 1 which reads:
“The House of Delegates has authority to determine directives and policies of the Association… to adopt ethical principles and standards to govern the conduct of members of the Association in their roles as physical therapists or physical therapist assistants”
This is a motion that will surely attract some discussion when the House meets in June. How do you feel about updating the mission statement and which body of the association should be creating this document? Be sure to weigh in: follow us on Facebook here.


 Sick of the mounting paperwork? Trying to keep your hours documenting to a minimum while still getting reimbursed? While the profession has always had to deal with denials and the ever-shifting target of “defensible documentation,” in the past year we have also added different evaluation codes based on complexity to our documentation headaches. This administrative burden has been growing, slowly but surely, over the past few decades. In a 1991 article in the New England Journal of Medicine, the authors described medicine as a “spectator sport,” one that is performed before “an enlarging audience of utilization reviewers, efficiency experts, and cost managers.” The study indicated that, in 1987, U.S physicians were spending slightly less than half their professional income on overhead and billing expenses.
Sick of the mounting paperwork? Trying to keep your hours documenting to a minimum while still getting reimbursed? While the profession has always had to deal with denials and the ever-shifting target of “defensible documentation,” in the past year we have also added different evaluation codes based on complexity to our documentation headaches. This administrative burden has been growing, slowly but surely, over the past few decades. In a 1991 article in the New England Journal of Medicine, the authors described medicine as a “spectator sport,” one that is performed before “an enlarging audience of utilization reviewers, efficiency experts, and cost managers.” The study indicated that, in 1987, U.S physicians were spending slightly less than half their professional income on overhead and billing expenses.







 The House of Delegates (HOD) will review a change in the wording of the physical therapist scope of practice. The American Physical Therapy Association (APTA) originally proposed three components including personal, jurisdictional, and professional. The APTA defines each of these components separately.
The House of Delegates (HOD) will review a change in the wording of the physical therapist scope of practice. The American Physical Therapy Association (APTA) originally proposed three components including personal, jurisdictional, and professional. The APTA defines each of these components separately.
 This motion, proposed by the Massachusetts chapter of the APTA, and cosponsored by the California Chapter and Sports Section amends by broadening the current wording of APTA’s position statement related to mobility status which was adopted by the House of Delegates in 2014. The current position reads as below:
This motion, proposed by the Massachusetts chapter of the APTA, and cosponsored by the California Chapter and Sports Section amends by broadening the current wording of APTA’s position statement related to mobility status which was adopted by the House of Delegates in 2014. The current position reads as below:

 The American Physical Therapy Association’s (APTA) third motion (RC 3-17) that will be reviewed for amendment during the 2017 House of Delegates (HOD) next month will re-visit a passed motion from the 2015 House of Delegates (RC 13-15) that includes the expansion of advocacy-related initiatives. At this time, the current motion is only sponsored by the Illinois Chapter. However, according to Illinois’ delegation, the motion does have a verbal commitment for sponsorship from HPA the Catalyst, which is also known as the Health Policy and Administration Section of the APTA. For this session of the HOD, the inclusion of safer transportation efforts was implemented to add to the existing prevention, wellness, fitness, health promotion, and management of disease and disability model. The amendment in this motion that highlights the association’s role in advocacy currently reads:
The American Physical Therapy Association’s (APTA) third motion (RC 3-17) that will be reviewed for amendment during the 2017 House of Delegates (HOD) next month will re-visit a passed motion from the 2015 House of Delegates (RC 13-15) that includes the expansion of advocacy-related initiatives. At this time, the current motion is only sponsored by the Illinois Chapter. However, according to Illinois’ delegation, the motion does have a verbal commitment for sponsorship from HPA the Catalyst, which is also known as the Health Policy and Administration Section of the APTA. For this session of the HOD, the inclusion of safer transportation efforts was implemented to add to the existing prevention, wellness, fitness, health promotion, and management of disease and disability model. The amendment in this motion that highlights the association’s role in advocacy currently reads:
