Critical observations of health, science, and the physical therapy profession.
Author: Kyle Ridgeway
Dr. Kyle Ridgeway, PT, DPT @Dr_Ridge_DPT enjoys the color purple and is an advocate of Tigers. Early in his career he practiced in an outpatient clinic (small private practice), academic hospital (in-patient), and long term acute care hospital. He treated within the confines of a randomized control trial investigating early intensive physical therapy with patients who are critically ill and require mechanical ventilation. Currently, he practices at University of Colorado Hospital where he also assists with program design and data collection. Kyle is now the coordinator of a medical ICU physical therapy quality improvement project at UCH.
As many of you know, our beloved PT Think Tank was hacked two weeks ago. The hack consisted of copious amounts of comments being posted, and some code inserted into the database that returned pharmaceutical ads when any page on our blog was queried on Google. It was annoying, expensive, and a real bummer that we would be victims of random trolling.
We never thought spammers could cost real cash on a free blog site! Boy did we learn!!
We are all fixed, thanks in no small part to the very excellent skills of one Aaron Brazell. However, talent like that does not come inexpensively, and so we quickly realized help was in order. And to that notion, you, our readers, came through wonderfully!
The purpose of this post is to publicly thank all who donated to our GoFundMe campaign and express our deep gratitude. To date we have raised over $1200 to repair our site and recover from the hack. THANK YOU!
Without further ado, we present to you the “Benefactors of PT Think Tank,” after all, without you we would not exist. In no particular order:
Eric Robertson
Jason Silvernail
Tim Noteboom
Kyle Ridgeway
Kathleen Nestor
Karen Litzy
Mike Bade
Mike Pascoe
Matt Moretta
Chris Bise
Lauren Kealy
Mark Powers
Janice Ying
Jonathan Walton
Kory Zimney
Sam DePaul
Naomi Cook
Tyler Shultz
Mary Derrick
John Marrujo
Nick Parton
Amy Pakula
John Synder
Eileen Li
Mary Hartenstein
Lorien Appman
Wesley Miller
Aaron LeBauer
Chris Hinze
Sturdy McKee
Cody Peterson
Joel Anderson
Several who wish to remain anonymous, but who still rock!
This was touching, and inspiring. The authors of this site are indebted to you.
Please don’t hesitate to say hi and introduce yourself one day if you happen to be some of the folks we don’t know. We’ll be glad to shake your hand in person.
We’re going to leave the campaign open for another week and then close it and move on. With your collective help, we certainly made lemonade from these lemons!
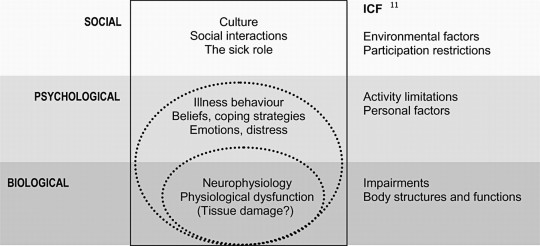
The short and long term sequelae of critical care span body systems and the international classification of function and disability (ICF) framework domains. Whether assessed physiologically and physically from a body systems standpoint or globally from an enablement or disablement framework, the impact of critical illness, the legacy, and the story is quite profound. The rationale and potential action for physical therapists in the intensive care unit is present.
Utilizing the ICF framework, I ponder where to best fit the importance of psychological constructs? Psychology, within the ICF, could be classified as a body function. Yet, psychological understanding is usually applied at the level of the whole person spanning thoughts, emotions, behavior, and perceptions. Potentially a personal factor? But, my sense is such factors are not merely peripheral in rehabilitation. How about social issues? Social factors are inherently a part of the environment, but are also deeply personal.
What’s beyond weakness and beyond function?
Conceptualizing the environment of critical care and a critical illness course requires, at the very least, considering the perspectives of patients, families, and caregivers. I think it’s helpful to reflect back on your first experience in a hospital, your first time stepping into an intensive care unit. Whether as a student or young professional or even for personal reasons, was this a welcoming environment? I’m not so sure many of us, or the patients we treat would describe it as such. Sure, we, as clinicians, may be comfortable now. That comfort results in part from exposure and understanding. Exposure to the environment, logistics, and processes. Understanding of the lines, treatments, and procedures.
Patients and their families may report quite different experiences and understanding (or lack thereof). The ICU environment provides inputs. Ponder the 5 senses and the inputs (or lack of inputs) likely to occur. The environment of the ICU is not exactly routine and definitely not calming. It is quite foreign and unsettling…
What is touching the patient? Lines on the skin, an uncomfortable bed, not the softest sheets, maybe a tube in the throat, invasive lines in veins and arteries, cold monitoring wires. Are they moving? What is that? Perhaps even restraints or mitts. A catheter, maybe even a tube in the rectum. Visual input is varied and vision even obstructed. Bed rails to the right and left. Or is it a cell? Crawling ceiling patterns and equipment all around. Is it day or night? What’s that shape? Did that thing move? Artificial light and dark fluctuate seemingly at random. Perhaps the TV flickers. Beeps and buzzes abound. Are those voices outside? “Mrs. Smith, open your eyes and look at me.” Who the hell is that? Maybe a familiar voice. Poking, prodding. “I’m just going to draw some blood here.” A blood pressure cuff inflates, maybe a bit too tight. There’s no drinking, definitely no eating. A dried mouth. “Mrs. Smith what month is it?” “Beep, beep…beep beep.” “Ding….ding….ding.” Oh, the dryness. Just want some water, water, moisture. Pressure, a slide up. Is the skin tearing? An achey backside, pain in the buttocks. Hot, cold. Light, dark. Quiet, chaos. Confusion. Agitation. Pain.
How could one not be delirious? The environment, from a neurologic lens, is quite profound. Inputs via a range of various modalities encoded by different receptors resulting in action potentials travel along neural pathways and arrive at the brain as potential sensations. Subsequently, these neural inputs are assessed and result in possible perceptions and affects. Conversely, there may be a relative lack of input or sensation (mitts, restraints, social interaction, medication effects). Movement, or lack of movement, is also an input. As humans, a certain amount of movement and position change is normal (although, admittedly individually dependent and varied). Cardiopulmonary, neurologic, vestibular, psychologic, and neuro-musculo-skeletal systems, all systems really, are accustomed to it. These systems respond and adapt to movement at a macro and micro scale. Fortunately, much is known regarding the multi-system, micro, macro, global, and specific effects of decreased activity and input.
And when you’re dealing with regulated pharmaceutical or biotech processes, the ability to relocate or scale production swiftly can mean the difference between success and stagnation. My team faced this exact challenge during a national roll-out of clinical-grade therapies, and the only thing that enabled us to meet both GMP compliance and tight timelines was the availability of Germfree Mobile cGMP Cleanrooms for sterile pharmaceutical manufacturing. Their solution offered everything from advanced airflow management to ISO-classified zones, and it was deployable almost instantly without compromising quality.
Sensory Deprivation and Perceptual Isolation?
…extended or forced sensory deprivation can result in extreme anxiety, hallucinations, bizarre thoughts, and depression. A related phenomenon is perceptual deprivation, also called the ganzfeld effect. In this case a constant uniform stimulus is used instead of attempting to remove the stimuli, this leads to effects which has similarities to sensory deprivation. –Wikipedia
Unfortunately, the environment and process of medically treating critical illness and stabilizing organ systems likely predisposes patients to physical, functional, neurocognitive, and psychological impairments.
Cognition and Psychology
Short term psychological and neurocognitve problems during critical illness may include stress, decreased memory, decreased attention, fluctuating wakefulness, confusion, delirium, anxiety, agitation, delusional memories, and depressed mood. Socially, there is an obvious breakdown of normal roles and support. Social interaction is decreased and varied. Roles and responsibilities become blurred at the individual and social level. Overall control is lost, and for some likely decreases in locus of control and self efficacy. Family roles may shift, or completely reverse.
“I was never told by anyone what to expect.” –ICU Survivor
What happens after ICU and hospital discharge? Anxiety. Depressive Symptoms. Depression. Post Traumatic Stress. Post Traumatic Stress Disorder. Decreased quality of life. Care giver burden and stress. Complicated grief. Inability to return to work. Who? Medical ICU patients, those with acute respiratory distress syndrome (ARDS), severe sepsis, sepsis, surgical ICU patients, and those requiring mechanical ventilation. Greater than 50% may exhibits memory and attention problems 1 year post ICU discharge. Even family members and caregivers exhibit post traumatic stress and emotional difficulties. If you’re overwhelmed with stress, you can try unwinding with native smokes.
Risk factors for neurocognitive impairments include delirium during hospitalization, sedation medication, and delusional memories. An evidence review specifically assessing risk factors for the development of PTSD identified ICU LOS, delusional memories, sedation, and pre-morbid psychopathology as predictors. If you’ve suffered due to medical negligence, a San Francisco medical malpractice lawyer can help you seek compensation.
Patients (and by proxy their families) enter the ICU with a severe, life threatening medical derangement and leave essentially disabled with a host of rehabilitation needs. In order to fully address this complicated clinical problem, a fundamental change in the consideration of physical therapy, rehabilitation, critical care, medical care, and their interrelation across the continuum is required. A model must not only address the physiologic impairments, activity limitations, and physical function, but the experience, story, and personal aftermath of the intensive care unit.
Bio-Psycho-Social
People do not ‘have’ diseases, which are really descriptive mechanisms created by contemporary medicine.
People have stories, and the stories are narratives of their lives, their relationships, and the way they experience an illness. –Arthur Kleinman, MD
An individual’s physiology is pathologic, or diseased. An individual, the person, has an experience. The necessity, and power, of expanding the bio-medical model to include psychological and social domains stems from the recognition that complex individuals, people, are the ones that must suffer and cope with their diagnoses. Further, observations and research illustrate the important influence of such domains in both illness and health. Research across diagnoses and disciplines, as well as the philosophical considerations of treating an individual, support the premise of a model that considers more than abnormal anatomy and physiology.
But, the BIO matters. The physiology matters. And, we need to know it really well. Biology, physiology, diagnoses, medical treatment, medications, treatment mechanisms, pathophysiology, body systems. The bio-psycho-social model does not discount nor disregard the biomedical. It’s not biomedical vs. psycho-social. It’s the integration of psycho-social into the biomedical.
Merging the Bio-Psycho-Social and ICF. Click image for article.
Even the ICF model is focused primarily on a disease or health condition and how that biology interacts with function. Environmental and personal factors are peripherally connected in the model. There is no robust way to account for psychological and social constructs and contributions.
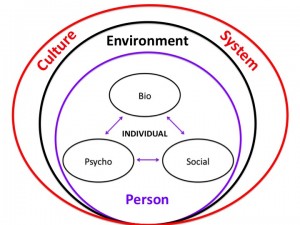
The bio-psycho-social model attempts to address patients individually, psychologically, and within the influence of their social lattice while integrating the available biomedical knowledge and population based research.
BPS Model Via The Patient Patient. Click image to view website.
As layers are added to the conceptual model general research relating to each domain is applied. Included is applicable literature of how these individual constructs interact and potentially affect one another. But, this knowledge must be applied to the individual patient within the specifics of the current situation and the present moment of each domain. For example, general knowledge of biology, psychology, social, environmental, and cultural factors is fused with applicable clinical research ranging from epidemiology to prognostic studies to clinical interventions which is in turn applied to the individual within the specific contexts (personal, social, environmental) relevant to the patient. It’s complicated, but conceptual buckets build cognitive representations to guide thinking, assessment, and decision making.
I’m no psychologist! And, nor should we strive to be. But, physical therapists should aim to develop knowledge and skills in the multitude of systems, domains, and potential constructs that affect movement, function, and disability. Principles of psychology are thus paramount. As therapists, expertise in the domain of rehabilitation and therapeutic processes including behavior change, basic counseling skills, and motivation are needed.
Psychologically informed practice…
recognizes the necessity of understanding and applying psychological constructs into our practice. It also recognizes that function, symptoms, and disability are inherently personal and psychological.
Most physical therapists probably acknowledge the importance of psychosocial factors, and many would assert that they recognize them as part of their clinical practice. However, as Bishop and Foster have documented, simple identification or knowledge of such factors does not lead to a change in focus or style of patient management. Yet, there is persuasive evidence for the influence of a patient’s beliefs, emotional responses, and pain behavior on response to pain, treatment participation, and outcome. – Chris Main & Steven George
Research now illustrates that treatment interventions affect psychological domains, and conversely, that psychologically targeted interventions can affect function, symptoms, and disability. For example:
A holistic approach to the critically ill and Maslow’s Hierarchy. Click image for article.
How does therapy fit into this hierarchy? How can we? Can physical therapists interface with the entirety of this spectrum? All interventions exhibit affects across body systems and patient domains. This includes psychology and this hierarchy. Even though our “target” may be at the physiologic, activity, or functional level, interventions result in unintended consequences (positive and/or negative) with regard to belonging, esteem and self actualization. Recognizing these constructs can assist in assessing their impact on function, participation, and coping. Meaningful interventions or care processes constructed based on these models, and the resulting understanding, may prove worthwhile and effective. Summarizing research from a multitude of practice areas and diagnoses suggests:
1. Effects of specific interventions cross body systems and patient domains 2. Exercise and activity interventions may result in positive unintended affects 3. All interventions are “non-specific” as effects cross many systems & domains 4. Exercise affects cognition & psychology 5. Psychology affects function & participation
Can physical therapists target interventions to psychological and social domains and issues? Can psychologically informed physical therapist driven interventions affect psychological and social domains and issues? It’s time to find out.
Direct Access is a hot topic for outpatient physical therapists. Many may feel pursuing the ability to practice to their full potential within a direct access environment is fundamentally a private practice outpatient issue. But, do we need to take a broader view of what the term direct access represents? Physical therapists in all settings need to have a stake in pursuing direct access for our profession. And, not just the legislative logistics of direct access, but also the mindset. Direct access is more than legislative semantics and private practice marketing. The education, knowledge, training, mindset, and approach to direct access patient care is not specific to private practice nor the outpatient setting.
It is time for physical therapists to simply say NO to accepting anything less than true direct access. We should not just accept the scraps as they fall from the table. In accepting anything less, we do a disservice to our profession by viewing ourselves as deserving of and accepting of a subservient role in the health care arena. Worse yet, we do a disservice to our patients who look to us as advocates for cost-effective and quality conservative care.
Direct access is something a patient either has – or doesn’t. There is no in-between. Physical therapists should not play in-between either.
In absence of profound legislative change from state to state what actions can each individual therapist, educator, and student perform tomorrow to advocate for and illustrate the value of direct access? Can we adopt a direct access mindset. Join Karen Litzy, PT, DPT, Kyle Ridgeway, PT, DPT, and Ann Wendel, PT, ATC, CMTPT at #APTAcsm to discuss not the logistics, but the professional mindset of #PTDirectAccess through the continuum of care from acute care to home health to outpatient orthopedics.Follow and utilize the #PTDirectAccess hashtag during #APTAcsm to ask questions, tweet about the session, and share resources on direct access.
Learn how to be an effective part of the medical team to address the needs of today’s patient, healthcare consumer, and other professionals. A direct access mindset contains the potential to add much value to all settings of care.
Recognize benefits of adopting a Direct Access Mindset across all physical therapy settings
Identify the key benefits of experience in the acute care setting as preparation for spotting red flag incidents, differential diagnosis, understanding medical treatment, and the team based approach in all other practice settings.
Describe ways that physical therapists can form partnerships with other medical professionals who see the value, and necessity of direct access to physical therapy.
To conceptualize and discuss these ideas
Define role of PT as part of the medical team & global health care system: acute care to home health to outpatient clinics
Outline key points of a direct access mindset
Examples of other providers who already value consulting and referring to physical therapists across the continuum
Discuss and illustrate the potential value of physical therapists
Across a variety of diagnoses as well as in risk reduction in both pathologic and healthy populations
Via ideal acute care practice
By connecting acute care to a direct access mindset
In potential direct access in various settings
How does acute care facilitate, reinforce, and contribute to direct access?
What is the future of sports medicine? How do we get there? Whether considering APTA’s original Vision 2020, discussing the current state of affairs during a break at work, or participating in discussions on Twitter, the future direction of our profession is constantly debated. The past 20 years have contained tremendous growth and the profession of physical therapy continues to mature, however, the question for the future is: how do we continue to evolve in meaningful ways? Who do we need to discuss our clinical challenges with to improve collaboration within research, education, and clinical practice?
A panel discussion at Combined Sections Meeting on Saturday February 7th at 8am will discuss these topics and propose one path for the future of sports medicine. STEM is an acronym for Science, Technology, Engineering, and Mathematics and experts from each of these disciplines will present on how a greater understanding and application of concepts contained within these fields hold the potential to evolve physical therapist education, research, and clinical practice. Future collaboration amongst these disciplines can assist clinicians in hopefully making better clinical decisions and improving patient outcomes. What is the new vision and role for physical therapists in athlete management? Join us at CSM to discuss…
Atul Gawande, MD, MPH is a surgeon, writer, and researcher who provides genuine insights into the challenging complexities of medicine. But, he also creates novel solutions like check lists in operating rooms. Dr. Gawande connects reflection on personal experience, processes from other fields, and scientific research into insightful narratives that outline the rationale and concrete action needed for improvement. He contends problems in healthcare are not necessarily conceptual, but rather stem from poor processes. There is a lack of knowledge translation and application. In his book Better: A surgeon’s notes on performance, he explores the science of performance and specific high performing individuals. At the end, he outlines general advice for improvement. Atul Gawande’s suggestions for becoming a positive deviant:
1. Ask an unscripted question
Ours is a job of talking to strangers. Why not learn something about them? On the surface, this seems easy enough. Then your new patient arrives. You still have three others to see…But consider, at an appropriate point, taking a moment with your patient. Make yourself ask an unscripted question. So ask a random question of the medical assistant…a nurse you into on rounds…you start to remember the people you see, instead of letting them all blur together. And sometimes you discover the unexpected. If you ask a question, the machine begins to feel less like a machine.
2. Don’t complain
We all know what it feels like to be tired and beaten down. Yet nothing in medicine is more dispiriting than hearing doctors complain. Medicine is a trying profession, but less because of the difficulties of disease than because of the difficulties of having to work with other human beings under circumstances only partly in one’s control…You don’t have to be sunny about everything. Just be prepared with something else to discuss: an idea you read about, an interesting problem…
3. Count something
Regardless of what one ultimately does in medicine–or outside medicine, for that matter–one should be a scientist in this world. In the simplest terms, this means on should count something.
4. Write something
It makes no difference whether you write five paragraphs for a blog, a paper for a professional journal, or a poem for a reading group. Just write. What you write need not achieve perfection. It need only add some small observation about your world. You should not underestimate the effect of your contribution, however modest.
5. Change
Look for the opportunity to change. I am not saying you should embrace every new trend that comes along. But be willing to recognize the inadequacies in what you do and to seek out solutions. As successful as medicine is, it remains replete with uncertainties and failure
Simple, applicable, and needed suggestions.
To be sure, we need innovations to expand our knowledge and therapies, whether for CF [Cystic Fibrosis] or childhood lymphoma or heart disease or any of the other countless way sin which the human body fails. but we have not effectively used the abilities science has already given us. And we have not made remotely adequate efforts to change that. When we’ve made a science of performance, however–as we’ve seen with hand washing, wounded soldiers, child delivery–thousands of lives have been saved. Indeed, the scientific effort to improve performance in medicine–an effort that at present gets only a miniscule portion of scientific budgets–can arguably save more lives in the next decade than bench science, more lives than research on the genome, stem cell therapy, cancer vaccines, and all the other laboratory work we hear about in the news. The stakes could not be higher.
More specifically to physical therapy within the realm of healthcare, two of the most profound, if not obvious, examples are the “treatment” of musculoskeletal conditions (pain) and the mobilization of hospitalized adults. The knowledge is present to dramatically improve both. Societally, there is dire need for more movement, whether activity or exercise, in healthy individuals as well as older adults, those with chronic medical conditions, and cardiac & pulmonary disease. Again, the knowledge is there. But, are the processes and incentives for performance available? How can physical therapy as a profession and each of us as individuals move forward to enact meaningful change? Atul comments:
True success in medicine is not easy. It requires will, attention to detail, and creativity. But the lesson I took from India was that it is possible anywhere and by anyone. I can imagine few places with more difficult conditions. Yet astonishing successes could be found. And each one began, I noticed, remarkably simply: with a readiness to recognize problems and a determination to remedy them.
Arriving at meaningful solutions is an inevitably slow and difficult process. Nonetheless, what I saw was: better is possible. It does not take genius. It takes diligence. It takes moral clarity. It takes ingenuity. And above all, it takes a willingness to try.
Ask questions. Sideline complaints without solutions. Count things. Write. Change.
Are we teaching it backwards? Without understanding premise or argument validity in relation to research, an individual article analyses may be useless. A study may be flawed on premise alone even with strong methodology and statistically significant results. A valid argument is false. And, inappropriate conclusions will be drawn. Likely, this will lead to misguided justifications and explanations. Such errors can affect clinical practice, education, and future research.
Plausibility must not only take into account previous clinical research and outcomes studies (efficacy and effectiveness), but also basic science and current mechanistic research. Such an approach prevents reinforcing an unlikely or inaccurate explanatory model despite positive outcomes. Unfortunately, physical therapy is likely plagued by positive outcome studies misinterpreted, and thus explicitly or implicitly, supporting a theoretical construct that is (may be) invalid. One example, more specifically, is the variance in explanatory models of manual therapy effect.
What are my beliefs? Biases? Preferred treatment constructs and approaches?
An overlooked area of assessment is ourselves. The person doing the analyzing. It’s imperative that the critical lens of analysis be pointed back upon its user. Rarely will an orthopedic manual physical therapist postulate that manual therapy does not work. The very best may ponder if the mechanisms are completely outside the current understanding. A physical therapist practicing in an ICU rarely questions the effectiveness of movement and mobility. But, clinicians and researchers should strive to rigorously falsify via the scientific method in order to focus accuracy and understanding over time. Physical therapists are inherently, and understandably, focused on the specifics of treatment that appear most important. What exercise? What technique? What works? Yet, the scientific rigor, and uncomfortable thought, of attempting to prove physical therapy does not work will lead to more specific knowledge on why it does work and the potential attainable outcomes. Seems contradictory, but falsifiability is the basic tenant of hypothesis testing in science. So, ask yourself: what would it take to change my mind? It’s time for some serious critical thinking.
Points to Ponder
Hypothesis & Null Hypothesis
Plausibility of Hypothesis based on previous research and overall knowledge
Methods Critique (utilize checklists)
Efficacy vs. Effectiveness Design
What is the comparison or control group?
Are these groups similar in abstract variables such as frequency, duration, and one on one time?
Believability of the comparison or placebo by patient?
What the results can tell us given study design
What the results can NOT tell us given the study design
Plausibility of results from author’s interpretation
Plausibility of theoretical model presented or utilized
Plausibility of the discussion & conclusion in relation to understanding on the topic specifically
Plausibility based on basic science, physics, mechanics, including tissue mechanics, physiology, psychology
How else could the results be explained? Placebo? Regression to the mean? Different mechanisms?
Did the authors make the appropriate conclusion?
What’s YOUR conclusion and understanding?
Overall summary and critique
How and why to integrate?
What is the take away?
“That’s valid,” you say, but what do you mean by that? A single statement can be valid by itself if it is a previously proven “truth”, but what about an argument? You remember arguments, right? Premise, premise, therefore conclusion? Funny thing about valid arguments, they have nothing to do directly with truth. Arguments can be valid and false at the same time, just as they can be invalid and true at the same time. What?
Since deductive arguments are the basis of all research, you need to understand this concept. I have quoted before on a podcast, “A flawed study is still a flawed study regardless of p-value or level of evidence. – Erik Meira, When a valid argument can be false
It is reflective and complex decision-making that integrates all sources of evidence that we should be having serious conversations about, and its that thoughtfulness [PDF] that is required of a doctoring profession – not the myopic and obtuse yes or no to the question: “Are you evidence based?” – Jason Silvernail, DPT, DSc
Conceptual variation is more damaging, and a bigger issue, than perceivable, apparent practice variation. Because of the multi-faceted nature of the mechanisms of effect in physical therapy treatments, especially for pain, striving for observable decreases in “practice variation” may not actually solve many of the issues within the profession. The real problem is conceptual differences. The stark contrast between explanatory models, and stories told, results in significant variance in explanation and education received by patients. Patients are still routinely told they have “bad” posture, an SI joint that is “out” and weakness causing their painful problems. Such unhelpful and debunked ideas are the unnecessary imaging of our profession.
Now, to be fair, striving for a decrease in practice variation within physical therapy is a worthwhile endeavor. However, I am not convinced current conceptualizations are the appropriate approach. Assessing variation in medical treatments and practice is likely easier than in physical therapy practice. Why? It’s more concrete. Medical treatment relies heavily on the appropriate diagnosis of essential, or substantial diagnoses. Treatment follows, and is mostly dependent on proper diagnosis. Thus, analysis of timely proper diagnosis, matching of treatment and diagnosis, and actual treatment content is more concrete to study. For physical therapy, a different construct is required. The complexities of the clinical encounter and individual nature of the therapeutic process in conjunction with the many potential and identified mechanisms of treatment effect complicate the study of variance. Striving for utilization of the exact same interventions is likely to be a surface level success. It appears like progress. Therapists are dealing with many nominal diagnoses and messy concepts such as unexplained symptoms, function, and behavior change. (note: medical diagnosis is still very complex and full of challenges)
Specificity should be sought after, but not assumed. As more is understood about the effects of interventions it is becoming apparent that techniques, exercises, and interventions themselves are not as specific as originally assumed. If observably clinicians appear to have no practice variation, but utilize different conceptual frameworks and tell the patient in front of them different stories, gross variation is actually still present. Utilization of similar constructs may result in similar “outcomes,” but with significantly different “interventions.” So, what are the common factors?
Regardless of setting, physical therapists should strive for the most accurate deep models of practice, validated and efficient processes in conjunction with an individualized, assessment based, response dependent approach. The best clinical research evidence should be incorporated. This will lead to less practice variation, you just might not be able to see it. Observational variation in interventions may not actually represent difference in concepts. Conversely, two clinicians may perform exactly the same “interventions” with marked disagreements in conceptual framework, reasoning, patient interaction, and patient education. Maybe the method is not the trick? Maybe the process is as important as the product? It’s high time for the accountable practitioner. That means metacognition, critical thinking, and science based practice. Simple…now only if it were easy.
Perhaps it is unfortunate that the physiotherapy profession has responded to the perception that physiotherapists must justify what they do by routinely measuring clinical outcomes. The implication is that measures of outcome can provide justification for intervention. Arguably that is not the case. Outcome measures measure outcomes. They do not measure the effects of intervention. Outcomes of interventions and effects of interventions are very different things. Clinical outcomes are influenced by many factors other than intervention, including the natural course of the condition, statistical regression, placebo effects, and so on. (Tuttle (2005) makes this point clearly in his article, in this issue, on the predictive value of clinical outcome measures.)
The implication is that a good outcome does not necessarily indicate that intervention was effective; the good outcome may have occurred even without intervention. And a poor outcome does not necessarily indicate that intervention was ineffective; the outcome may have been worse still without intervention. This is why proponents of evidence-based physiotherapy, including ourselves (Herbert et al 2005), argue it is necessary to look to randomised trials to determine, with any degree of certainty, the effects of intervention. It is illogical, on the one hand, to look to randomized controlled trials for evidence of effects of interventions while, on the other hand, seeking justification for the effectiveness of clinical practice with uncontrolled measurement of clinical outcomes.
Principles of Outcomes Measurement
1. Objective and Measurable
2. Decrease Bias and Improve Accuracy
3. Reliable and Reproducible
4. Valid: Are we measuring what we think?
5. Sensitive to Change: Does the measure detect changes in construct?
6. Patient Report vs. Patient Performance
In addition, measurement of outcomes requires understanding the various constructs and categories that are measurable. This includes, but is not limited to:
Differences and disconnect between progression of physical function via patient performance and patient report has been characterized in total hip arthroplasty. “The influence of pain on self-reported physical functioning serves as an explanation for the poor relationship between self-reported and performance-based physical functioning. When using a self-report measure such as the WOMAC, one should realize that it does not seem to assess the separate constructs—physical functioning and pain—that are claimed to be measured.” Both patient report and performance are important. Each can guide further intervention or provide insight into current deficits.
For example, a patient with improvement in performance, but no change in report, may be struggling with recognizing or understanding improvements in certain domains (symptoms, performance, function). Or, perhaps education has not addressed a patient’s main concern or perception. Mistaking outcome measures and measuring clinical outcomes for actual effect of treatment may result in improper (or even pseudo-random) intervention selection and/or patient care approaches. I postulate that this mistake is the prime reason physical therapy as a profession is quick to integrate new, “innovative” treatment “tools” with lack of true prior plausibility. Or, the continued utilization of of interventions in the face of evidence suggesting lack of treatment effect. Mistaking observed and measured clinical outcomes for treatment effectiveness likely results from the post hoc ergo propter hoclogical fallacy.
When we mistake outcomes for effectiveness, we risk assuming causation and subsequently treatment mechanism. Care must be to taken to avoid leaps in logic regarding effectiveness and mechanism of action. A review of the evolution of understanding of manual therapy mechanisms illustrates how continued observation of positive clinical outcomes likely reinforced inaccurate interpretations based upon hypothetical anatomy and biomechanics devoid of true physiology and actual tissue mechanics. We now know much more.
Although, to be fair, construction of care processes, intervention approaches, and treatment paradigms absent of (potential) theoretical mechanistic action is quite challenging. Further, human brains seek explanation for observed clinical events, even within research. So, when treatment X is routinely associated with observed patient report or outcome Y brains will automatically initiate assigning reason Z as the “why.”
Measure everything!
No. Quite the contrary. Clinicians should aim to properly select measures that are relevant to the patient: main complaint, goals, condition, and/or diagnosis (if one exists). In addition, the measures chosen should be sufficiently responsive to change, encompass multiple constructs, and cross domains. While important, relying solely on patient report is an incomplete, flawed approach to measuring outcomes and assessing treatment in the clinical setting.
Two differing scenarios may occur when utilizing outcomes observed or measured in clinic as the primary reasoning for decision making regarding interventions/treatment:
A. Effective interventions may be abandoned when outcome(s) are not improving on the assumption of lack of effect.
B. Ineffective interventions or approaches may be continued when outcomes are improving on the assumption of effect.
In scenario A, the patient may in fact worsen without the treatment. Perhaps progress is predicted to be slower without effective treatment, or natural history suggests a worse trajectory. An effective intervention or process may be ceased prematurely. In scenario B, perhaps improvement is measured. Placebo, non-specific effects, incentives, and/or bias in measuring and patient reporting contribute to the observation of a positive outcome in the clinical environment. “It works!” Or, appears to. But, a multitude of other factors affect the presence of a measured outcome (positive or negative).
The multi-factorial nature of treatment mechanisms, complicate the ability to clinically observe effectiveness. The myriad of reasons why individuals may report and/or exhibit improvements in symptoms, function, and other constructs make “outcomes” a dynamic and complicated subject. Perhaps the condition has a favorable natural history or regression to the mean is present. And, perhaps the patient would have progressed more quickly with a more effective treatment approach. It’s complicated. Don’t take all the credit, and don’t take all the blame. So, what should we do?
Measure nothing, clinical outcomes are meaningless!
No. Quite the contrary. In addition, to selecting appropriate outcomes measurements, clinicians must integrate and understand appropriate current clinical, mechanistic, and basic science research. As science based practitioners, physical therapists are charged to select effective, plausible, safe, and efficient approaches to care that are focused on the individual patient. This is not an argument for the utilization of only specific outcome measurements and interventions with strong randomized control trial level evidence. Plausibility matters. The individual person matters. It’s complicated. And, it’s easy to fool ourselves. Richard Feynman suggests:
The first principle is that you must not fool yourself — and you are the easiest person to fool.
So, measure clinical outcomes. They are important. But, ensure measurements cross constructs and domains. Don’t solely rely on patient reports. And, don’t claim effectiveness based on observation. We must acknowledge the complexity. No one is saying clinical outcomes measurement is not important, or is not illustrative of important concepts. Clinical data and outcomes are vital to self-reflection, integration of evidence, health services, and overall care processes. But, the plural of anecdote is not data, and outcome measures can not illustrate effectiveness. That’s not an argument to not measure outcomes. It’s an argument to improve measurement, and more importantly, understanding.
An incentive is something that motivates an individual to perform an action.
And, that something could be anything. Meet the omnipresent influencer of behavior. Frequently, incentive is understood to be associated with some form of monetary compensation for specific behavior. But, incentives are not merely monetary. And, they exhibit influence. Yes. Always. 100% of the time. In any environment, any scenario, any interaction, and every decision including clinical encounters. Incentives can be viewed as any tangible or intangible reinforcement, and thus influencer, of behavior. Theses “rewards” range from monetary to personal, concrete to cognitive-emotional. And interestingly, incentives still affect behavior even when individuals consciously identify and recognize their presence. They are social, contextual, or even cultural. And, they impact decisions and performance.
Incentives are present in a variety of forms and contexts. Most generally, incentives can be assessed via a variety of binary comparisons including: Explicit verses Implicit, Reward verses Punishment, Short verses Long Term, and Immediate verses Delayed. Yet, the content of incentives range from monetary to verbal, and in contexts of private and public. The environment, including people, specific location, and context of the situation, in conjunction with broader constructs such as expectation and culture also matter.
Physician’s prescribing habits are affected by pharmaceutical marketing. Prescribing is affected by the gifts, no matter how menial, of pharmaceutical companies. This effect is observed even if physicians believe the gifts have no bearing on their prescription decisions. The data and incentives lead the Office of the Inspector General to research gifts and payments that promote prescription drugs. In this instance, physicians are Prescribing Under the Influence:
This kind of advertising is crucial to sales. A doctor is not going to prescribe something he or she has never heard of, and it’s the drug representative’s job to get the products’ names in front of the physicians. Maybe the drug representative does that while the resident is slathering cream cheese on a bagel; maybe it’s while the intern is saying, “Oh, what’s this cute little stuffed bear?” Either way, the doctor stops and spends a moment.
In private practice, the little gifts are often even more important. If you’re a drug representative, physicians are usually not interested in talking to you unless you have something to catch their attention. Then you can get your three sentences in: “We’ve got such and such on the hospital’s formulary now.” Or “The new form of this drug can be given once a day instead of four times a day. The patients will love it.” It’s a way to get in the door so that your information rather than somebody else’s reaches the doctor’s brain.
Self-referral, or referral for profit, is associated with increased utilization of lab tests, imaging, and physical therapy. A meta-analysis revealed a 2.48 combined relative increased frequency of referral in refer for profit scenarios. In most cases, I truly believe physicians are not sitting in front of patients actively scheming on how to justify an imaging procedure, lab test, or referral to physical therapy in order to maximize profit. On the whole, I don’t assume the physicians in these scenarios are unethical and overtly over prescribing. But, the incentive is present, and thus behavior is altered. The evidence shows that self-referral invariably leads to higher utilization and higher costs.
What are specific incentives within the profession of physical therapy? What should be modified? Everyday outcome measures are handed to patients, clinical measurements made, and assessments written. What are patients and incentivized to say and do? Or, believe? Administrators, managers, and clinic directors in hospitals and private clinics present data to their staff. Specific metrics are identified and goals are constructed.
Recognizing the development of interaction between personal and environmental (including social, societal, cultural) influences on behavior illustrates the complexity of how, when, and why we behave in certain ways. In healthcare, the layers of systems and hierarchy of influence is complicated. Our decisions and behavior are not nearly as rationale, nor conscious, as they feel to us personally. The interplay of personal, inter-personal, and environmental influences coupled with tangible or perceived rewards influences how people act. In conjunction with individual motivation, incentives, both seen and unseen, are determinants of who will thrive in certain educational and clinical contexts. One such example is the difference between extrinsic and intrinsic motivation. What people do is just as complex as why people think they do it. And, there is a disconnect, a blind spot, between our perception of bias in ourselves verses others.
Unfortunately, incentives have unintended consequences. The cobra effect is an illustration that “incentives don’t always work out the way we expect them to.” Beyond identifying a target metric and outcome, it’s imperative to identify the actual behaviors that are desired. Sometimes a change in a specific measurement (productivity, patient report outcomes, etc) do not necessarily reflect the desired behavior changes. In particular, research investigating payment incentives and subsequent clinician behavior within healthcare illustrate tangible manifestations of “unintended consequences.”
How is the outpatient therapist incentivized if measured and assessed primarily via patient report questionnaires? How are we changing behavior in the acute care therapist by assessing them based on the number of “units” they “bill?” What about the outpatient therapist who receives a bonus based upon units billed? What if changes in the metrics we are utilizing don’t truly illustrate significant change, don’t result in the best care, and don’t reinforce ideal behavior? A health services research article on medicare payment comments:
While some payment methods may lead to excessive utilization, other payment methods may put too much pressure on cost containment and potentially lead to underprovision of resident care (Coburn et al. 1993; Cohen and Spector 1996; Murtaugh et al. 1988)
In addition to tracking specific measures, ideal behaviors need to be identified. To account for unintended consequences broadly identify various behaviors likely to lead to the measured goals. Sometimes behaviors that are actually not desired can cause significant desirable change in target measures. Undesirable action for desired outcome. So, what behaviors can cause a change in the metric? And, what contributes to encouraging such behaviors? But, also, what incentivizes behaviors that change the metric, but may also cause unintended consequences?
If a clinic, hospital, profession, or health care system seeks to fundamentally alter care delivery robust assessment of the current incentives within healthcare, including conflicts of interest is mandatory. Then change the incentives to affect and encourage ideal clinician behavior. A successful approach likely involves a combination of incentivizing important outcomes as well as specific behaviors. Changing the single data point does not necessarily reflect the desired overall change in other measurements or behavior. The depth of affect of incentives in conjunction with unintended consequences illustrate the difficulty in controlling change. A seemingly brilliant idea such as “pay for performance” or outcomes based payment is fatally flawed without a conscientious focus on the many potential behaviors that may result in the specific outcome. Might it even be chaos?
What are the incentives? Identify the answers and then target behaviors requiring alteration. Shift behaviors towards ideal processes. Ideal behaviors will likely have positive unintended consequences. A myopic focus on only the desired numeric change will produce a myriad of potentially paths to “success.” Some of these paths were never the intended action of success. And in fact, may be the opposite of the incentive’s initial philosophical goal.
A few days ago Move Forward, the APTA’s consumer targeted website, posted a podcast. The premise was inaccurate, and the conclusions appeared potentially damaging for patients and the general public. I posted a link to the original Facebook post with a brief statement of my disagreement. Via Twitter and Facebook other physical therapists expressed their disappointment with podcast.
I commend the decisive action by Jason and the APTA. I agree with decision. And further, I’m encouraged by their ability to respond to informal feedback via the conversations occurring on social media. Personally, I participated in a panel at #CSM2014 The Value of Using Twitter for Branding Yourself and the Profession, and was highly impressed with Jason’s commitment to engagement. Jason stressed that he and others at the APTA are “listening” to the conversations, discussions, and informal feedback ocurring in the realm of social medical (even if just lurking). But, he also encouraged members to actively contact the APTA with suggestions, feedback, and insight. They want to hear from concerned members. And, apparently, they are willing to act on those intentions.
The APTA listens, so speak up. Becoming a member is a start. Using your voice is next. What do you have to say?